Open Disclosure Process
Conducting an open discussion with a client about an incident that resulted in harm while they were receiving care.
It is not intended that all steps and actions be completed in exact order in every situation.
Open disclosure is a very complex and sensitive undertaking and can be a difficult process. As such, there is not one standardised way to conduct open disclosure. Flexibility is required to meet specific circumstances and the needs of clients and workers.
These policies and procedures are adopted to ensure appropriateness to the home care environment.
Note: All discussions should regard the ethical and legal requirements relating to confidentiality and privacy of clients and clinicians.
It is not intended that all steps and actions be completed in exact order in every situation.
Open disclosure is a very complex and sensitive undertaking and can be a difficult process. As such, there is not one standardised way to conduct open disclosure. Flexibility is required to meet specific circumstances and the needs of clients and workers.
These policies and procedures are adopted to ensure appropriateness to the home care environment.
Note: All discussions should regard the ethical and legal requirements relating to confidentiality and privacy of clients and clinicians.
Detecting and Assessing Incidents
Key considerations and actions
- Detect incidents through a variety of mechanisms
- Provide prompt clinical and personal care to the patient to prevent further harm
- Assess the incident for severity of harm and level of response
- Provide support for workers
- Initiate a response ranging from lower to higher levels
- Notify relevant personnel and authorities
- Ensure privacy and confidentiality of clients and clinicians are observed
Open disclosure begins with recognising that the client has suffered harm during care.
Identifying an adverse event
Identifying an adverse event
An adverse event might be identified:
- by a CCM or worker at the time of the incident
- by CCMs retrospectively when an unexpected outcome is detected
- by a client, their family and carers at the time of the incident or retrospectively
- through established complaint mechanisms
- through incident detection systems, such as incident reporting
- from other sources, such as detection by family, visitors or other staff.
All incidents must be considered, regardless of the mechanism through which they were detected.
Supporting the client and CCM as a priority
Prompt and appropriate clinical care and prevention of further harm are prioritised as soon as harm is identified. Additional treatment should be provided if required and reasonably practical after discussion and with the client's agreement.
The Principal - Clinical Governance (PCG) should be advised and should gather any evidence that will assist in investigating the event. This should occur in consultation with the clinical risk team and executive where appropriate.
The Principal - Clinical Governance (PCG) should be advised and should gather any evidence that will assist in investigating the event. This should occur in consultation with the clinical risk team and executive where appropriate.
CCMs (and other staff) involved in the adverse event should be monitored and supported as required.
Initial assessment to determine the level of response
The person who detected the incident should make an initial assessment of the incident, usually in consultation with a CCM. This process will consider the severity of harm and the level of response required.
The level of response required will be determined by the incident's effect, severity or consequence, as described in the next section.
The level of response required will be determined by the incident's effect, severity or consequence, as described in the next section.
Lower and higher‑level responses
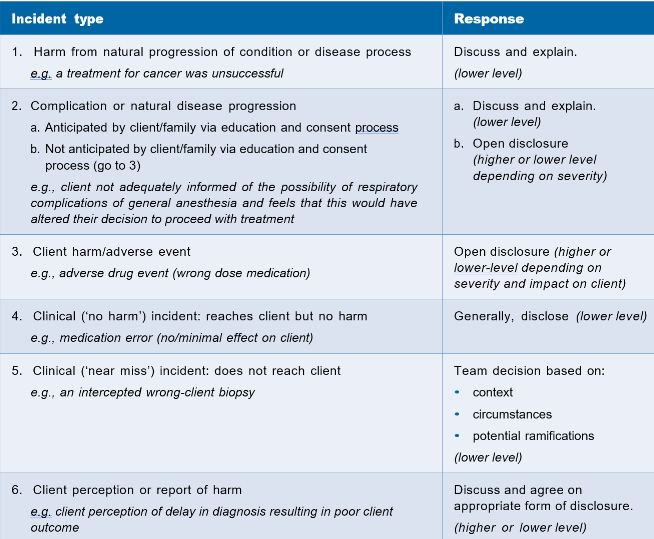
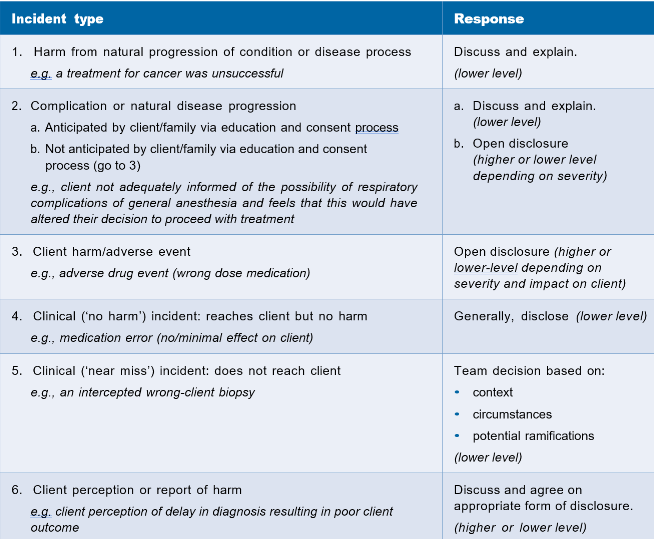
The incident's effect, severity or consequence will determine the incident response. Examples of incident types and suggested responses are described in the table below.
{kind=link}
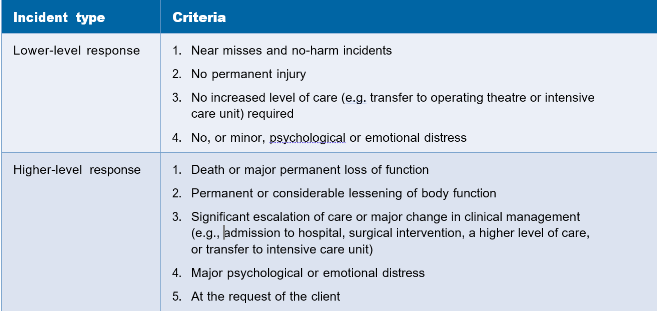
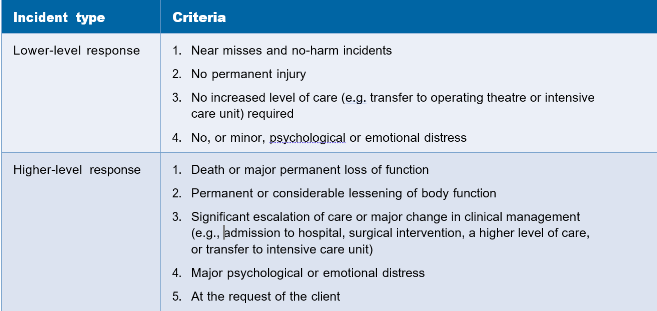
The following table describes lower and higher-level responses linked to criteria for harm that may be used to delineate lower and higher-level responses.
It is important to consider that clients and their families can suffer further emotional harm if post-incident communication is managed insensitively. A lower-level response should only be initiated if the risk of further harm (from not conducting higher-level open disclosure) is unlikely.
Where uncertainty exists, a higher-level response should be initiated.
{kind=link}
Adverse drug events
Medicines are the most common therapeutic intervention in Australia. While most medicines are
delivered safely, their use and delivery carry inherent risks, and it has been estimated that over 1.5 million Australians suffer an adverse drug event (ADE) each year.
Where ADEs result from omission or the administration of the wrong dose, the criteria above should guide the appropriate level of our response.
Delayed detection of harm
In some cases, client harm may not be detected for some time. These adverse events may have occurred elsewhere. It is important to consider the principles of open disclosure in these situations. In this situation, we should:
- Notify the client and their family of what has occurred
- Inform their other healthcare providers, such as their general practitioner, of the incident
- Notify the CCMs who were involved in the incident
- Commence an investigation of the incident and establish the facts.
Open disclosure should then proceed based on the circumstances outlined in our Open Discussion Framework. The CCMs involved in the incident should participate in the open disclosure process.
The process must adapt to the client's needs, family, workers, and CCMs. For instance, open disclosure meetings may occur in a suitable location or by videoconference.
Device safety
Technological advances are introducing increasingly complex instruments, implants and devices in health care.
Incident detection systems and mechanisms should be continually updated to ensure harm caused by a failure and malfunction of medical devices (as opposed to their incorrect usage or application) are captured, triggering open disclosure and notifying the responsible organisation(s).
Incident detection systems and mechanisms should be continually updated to ensure harm caused by a failure and malfunction of medical devices (as opposed to their incorrect usage or application) are captured, triggering open disclosure and notifying the responsible organisation(s).
Signalling the need for open disclosure
Key considerations and actions
- Acknowledge the adverse event to the client, their family and carers, including an apology or expression of regret.
- A lower‑level response can conclude at this stage
- Signal the need for open disclosure
- Negotiate with the client and their family or nominated contact person
- the formality of open disclosure required
- the time and place for open disclosure
- who should be there during open disclosure
- Provide written confirmation
- Provide a health service contact for the client and their family.
- Avoid speculation and blame.
- Maintain good verbal and written communication throughout the open disclosure process.
The initial discussion
The initial discussion should occur immediately after recognising harm, even if all the facts are unknown. During the initial discussion:
- the adverse event is acknowledged to the client and their family
- an apology or expression of regret is given (see Sections 1.5 and 10.2)
- the effect of the incident, including all known facts and the consequences, are described.
The disclosure process will likely be completed after the initial discussion if a lower-level response is indicated.
An example of appropriate wording for a lower-level response initial discussion is
An example of appropriate wording for a lower-level response initial discussion is
‘I am/we are very sorry that this has occurred. It is clear that something unexpected has occurred/things didn’t go to plan but fortunately it was recognised immediately and we have ensured that you did not suffer any harm from it. However, we will keep an eye on you for the next 24 hours and will ask you to let us know if you feel anything unusual. We do not expect that you will need to stay here any longer than originally planned.’
The person conducting the initial discussion may be one of several health professionals and CCMs. The circumstances should determine this.
Unless there are specific indications, or the client and their family request it, the open disclosure process will occur at the home with the participation of those directly involved in the incident.
Where relevant, reporting to management will occur through standard mechanisms consistent with local clinical governance, risk management and quality improvement policy and practice. These reports should be analysed to detect high-frequency events.
The initial discussion will have two additional actions if a higher-level response is indicated.
- Signal the need for open disclosure.
- Negotiate (where possible) with the client and their family about:
- the format required for discussions and meetings
- the logistical details of the open disclosure.
An example of appropriate wording for a higher-level response initial discussion is:
‘I am/we are deeply sorry that this has occurred. It is clear that something went wrong and we are investigating it right now. We will give you information as it comes to hand. It is very important for us to understand your version of what happened. We can go through this now if you like, or we can wait until you are ready to talk about it.’
Avoiding speculation and blame
It is important not to speculate, attribute blame to yourself or others, criticise individuals or imply legal liability when signalling the need for open disclosure or during formal open disclosure discussions. All known facts relevant to the adverse event can be made available to the client, their family and carers subject to any legal restrictions that may apply (see Appendix 1).
Maintaining good internal communication throughout the process
Good internal communication is critical throughout the period the open disclosure process takes place. The absence of good communication can result in the client and their family receiving conflicting information and mixed messages.
Preparing for open disclosure
Key considerations and actions
- Hold a multidisciplinary team discussion to prepare for open disclosure
- Consider who will participate in discussions
- Appoint an individual to lead the open disclosure based on previous discussions with the client and their family.
- Gather all the necessary information.
- Identify the health service contact for the client and their family (if this is not done already)
Team Discussion
Where appropriate and relevant, the multidisciplinary team and all CCMs involved in the adverse event, including the PCG, will communicate as soon as possible after the event to achieve the following.
- Establish the basic facts (clinical and other facts).
- Assess the event to determine the appropriate response.
- Identify who will take responsibility for the discussion with the client and their family (see below).
- Consider the appropriateness of engaging client support early on, including using a facilitator or a client advocate.
- Identify immediate support needs for everyone involved.
- Ensure that all team members maintain a consistent approach in discussions with the client and their family.
- Consider legal and insurance issues for the organisation and the CCMs, and notify the relevant people.
- Consider how to address issues regarding ongoing care, such as invoicing and other costs, which should be addressed at the earliest opportunity.
Note: The composition and conduct of the team discussion depends on organisational size and may only sometimes be appropriate.
The client record must be up to date before the team discussion takes place.
Choosing who leads the disclosure
Choosing who leads the disclosure
The individual leading the disclosure should be the PCG or if unavailable the CCM responsible for the client's care. Ideally, the lead person should:
- be known to the client and their family
- be familiar with the facts of the adverse event and the care of the client
- be of appropriate seniority to ensure credibility
- have received training in open disclosure
- have good interpersonal skills
- be able to communicate clearly in everyday language
- be able and willing to offer reassurance and feedback to the client and their family
- Where possible and appropriate, be willing to maintain a medium to long-term relationship with the client and their family.
The decision about who will make the disclosure should, where possible, be made in consultation with the client and their family, clinical risk personnel and (if appropriate) senior management (in relevant health service organisations).
If, for any reason, the PCG cannot lead the open disclosure, a substitute will need to be selected, but ideally, the PCG should still be present at the discussion.
If, for any reason, the PCG cannot lead the open disclosure, a substitute will need to be selected, but ideally, the PCG should still be present at the discussion.
The person leading the open disclosure may require the support of a senior staff member with appropriate skills.
Deferring open disclosure
Prompt open disclosure may not be indicated in every situation and may need to be deferred in some instances. For example, if the physical or mental health of the client is not conducive to participating in open disclosure, the process may need to be deferred. The client and their family may also request a deferral.
In these exceptional cases, a decision not to disclose can be justified as being in the client’s best interest. In these cases:
- The rationale must be documented in the client record
- A clinician or colleague not involved in the adverse event should independently verify the decision. This verification must also be documented in the client record.
If open disclosure is deferred with the client but is held with the client’s family, carers or other relevant persons, the process should recommence with the client later.
Arranging the first meeting
Timing, location and attendees
The timing and location of the first face-to-face open disclosure meeting should be decided in consultation with the client, their family and workers. Conducting the open disclosure where the harm occurred may not be appropriate. In these cases, other arrangements should be considered. Videoconferencing may also be appropriate.
The client and their family should be consulted about which CCM and staff will participate in the open disclosure meeting.
Factors to consider include the following:
- client’s clinical condition
- availability of key staff
- availability of the client’s family and carers and other relevant support persons
- availability of support for staff
- client’s preferences (and those of their family and carers)
- client’s privacy and comfort
- client’s physical and mental health.
The client and their family may need time to consider these matters.
If, for any reason, it becomes apparent that the client and their family would prefer to speak to a different CCM than those designated to lead the open disclosure, the client’s wishes should be respected and, if possible, an acceptable substitute provided.
Health service contact
The client and their family should be provided with the name and details of a health service contact who should provide information and support to the client and relevant persons throughout the open disclosure process and manage the open disclosure to its completion. Only one person should fulfil this role throughout the process, and it is recommended that they should not have been directly involved in the incident.
The client should identify their nominated contact person if they still need to.
Written information
The client and their family should be given written information on open disclosure in a language or communication style they understand if this has yet to be done at the time of admission. The information should be provided in an appropriate format.
Engaging in open disclosure discussions
Key considerations and actions
- Provide the client, their family and workers with the names and roles of all attendees.
- Provide a sincere and unprompted apology or expression of regret, including the words
- I am or
- we are sorry
- Clearly explain the incident.
- Give the client, their family and carers the opportunity to tell their story, exchange views and observations about the incident and ask questions.
- Encourage the client and their family to describe the personal effects of the adverse event.
- Agree on, record and sign an open disclosure plan.
- Assure the client and their family they will be informed of further investigation findings and recommendations for system improvement.
- Offer practical and emotional support to the client and their family and Support staff members throughout the process.
- Support staff members through the process
- If the adverse event occurred in another health service organisation, include relevant staff if possible.
- If necessary, hold several meetings or discussions to achieve these aims.
Open disclosure will usually occur over the course of several discussions. The first open disclosure meeting may be the first part of an ongoing dialogue and communication process.
Key components of open disclosure discussions
The key components of open disclosure discussions are listed below.
- The client and their family are told the name and role of everyone attending the meeting, and this information is also provided in writing.
- A sincere and unprompted apology or expression of regret is given on our behalf and CCMs, including the words ‘I am’ or ‘we are sorry’ (see Sections 1.5 and 10.2). Examples of suitable and unsuitable phrasing of an apology are provided in Box 3 in Section 10.2.
- A factual explanation of the adverse event is provided, including its known facts and consequences, in a way that ensures the client and their family understand the information and consider any relevant information related earlier by the client and their family. Speculation should be avoided.
- The client and their family can tell the CCMs their story about the adverse event to explain their views on what happened, contribute their knowledge and ask questions (the client’s factual explanation of the adverse event). It will be important for the client and their family that their views and concerns are listened to, understood and considered.
- The client and their family are encouraged to talk about the personal impact of the adverse event on their life.
- An open disclosure plan is agreed upon and recorded in which the client and their family outline what they hope to achieve from the process and any questions they would like answered. This should be documented and filed appropriately, and a copy should be provided to the client and their family.
- The client and their family are assured that they will be informed of any further reviews to determine why the adverse event occurred, the nature of the proposed process and the expected time frame. The client and their family are given information about how feedback will be provided on the investigation findings, by whom and in what timeframe, including any changes made to prevent recurrence.
- An offer of support to the client and their family should include:
- ongoing support, including reimbursement of out-of-pocket expenses incurred as a result of the adverse event
- assurance that any necessary follow-up care or investigation will be provided promptly and efficiently
- in relevant settings, clarity on who will be responsible for providing ongoing care resulting from the adverse event
- contact details for services they may need to access
- information about how to take the matter further, including any complaint processes available to them.
- The client and their family openly disclose with staff. Staff are supported by their colleagues and managers personally (emotionally) and professionally (including through appropriate training, preparation and debriefing.
- In cases where the adverse event spans more than one location or service, health service staff will ensure that, where possible, all relevant individuals from these additional institutions are involved in the open disclosure process.
It is optional to cover every component in the first disclosure meeting. For instance, explaining why an adverse event occurred may only be possible once the causative factors are known.
A written account of the open disclosure meeting should be provided to the client and their family.
How to make an apology or expression of regret
As relevant and appropriate, the person(s) apologising or expressing regret during open disclosure should include the following.
- Acknowledge that an adverse event or something didn’t go as planned.
- Acknowledge that the client and family are unhappy with the outcome.
- Apologise or express regret for what has occurred (including the words ‘I am/we are sorry’).
- Provide known clinical facts and discuss ongoing care (including any side effects to be aware of).
- Indicate that a review or investigation will be undertaken to determine what happened and prevent the adverse event from happening again.
- Agree to provide feedback information from this when available.
Examples of appropriate phrases during an apology
- ‘I am/we are sorry for what has occurred.’
- Factual statements explaining how the incident occurred
- ‘This incident occurred because the wrong label was mistakenly placed on your specimen sample.’
- Explaining what is being done to ensure it does not happen again
- ‘We are currently investigating exactly what caused this breakdown in the process and will inform you of the findings, and steps taken to prevent recurrence, as soon as we know.'
Examples of phrases to avoid during an apology
- ‘It’s all my/our/his/her fault … I am liable.’
- ‘I was/we were negligent …’
- Any speculative statements.
Providing follow-up
Key considerations and actions
Key considerations and actions
- Ensure follow-up by the PCG or CCM where appropriate
- Agree on future care
- Share the outcomes of investigations and the resulting practice changes
- Offer tthe client and their family the opportunity to discuss the process with another clinician (e.g. a general practitioner)
Follow-up with the client and family is important in higher-level responses to open disclosure. Lower-level responses may require no or minimal follow-up.
Key components of follow‑up
Key components of follow‑up
The senior CCM involved in the adverse event (or PCG, if appropriate) should be involved in the follow-up discussion, which should occur at the earliest practical opportunity. The client and family should be assured of receiving further information and follow-up care and be readily provided with any information they request (without contravening legal constraints).
They should also be informed of the progress and results of any investigation, including whether the results are delayed, pending or uncertain. We should notify the client and their family of any changes to practice intended as a result of the investigation and the changes that have been made to prevent the recurrence of the adverse event.
The client and family should be offered an opportunity to discuss the situation with another relevant professional, where appropriate. This may include involving the general practitioner, in the discussion, with the client’s permission.
The client and family should be provided with details of a person to contact if further issues arise.
Completing the process at this stage
If the process of open disclosure is complete at this point, the client and family should be asked if they agree that the process is complete, and a note of this should be made in the client's record. Written information about the adverse event and its management should be provided to the client and family.
The client and family should be offered an evaluation survey or, where it is considered more appropriate, a face-to-face interview or both.
Completing the process
Key considerations and actions
- If appropriate, agree between the client and their family or provide an alternative course of action.
- Provide the client and their family with final written and verbal communication, including investigation findings.
- Communicate the details of the adverse event, and outcomes of the open disclosure process, to other relevant clinicians.
- Complete the evaluation surveys.
The open disclosure process concludes with the shared agreement between the client, family, and us. This will occur most after the adverse event incident review or investigation.
If a satisfactory conclusion cannot be negotiated, the client and family should be offered alternative courses of action.
Key components for completing the process
Communication
When the relevant review or investigation is complete, the client and family should receive feedback through a face-to-face interview or equivalent (e.g. videoconference) and in writing. The interview and document should include the following.
- Details of the incident, including the clinical facts and other relevant facts.
- The client’s concerns or complaints.
- An apology or expression of regret (including the word ‘sorry’) for the harm suffered.
- A summary of the factors contributing to the adverse event.
- Information about what has been and will be done to avoid the recurrence of the adverse event and how these improvements will be monitored.
If further issues are identified after the process is completed, the client and family can re-contact the health service organisation for a response to their questions.
Disclosure of review and investigation findings
In most cases, the findings of relevant reviews or investigations will be completely disclosed. A formal, written report should be provided in a language and communication style that the client and family will understand.
In some exceptional circumstances, it may be considered that disclosure of information will adversely affect the client and family’s health. In these cases:
- The rationale must be documented in the client record
- Where possible, a practitioner or colleague who was not involved in the adverse event should independently verify the decision. This verification must also be documented in the client record.
In addition, in some cases and jurisdictions, information may be withheld or restricted. This may occur, for example, where:
- investigations are awaiting the conclusion of coronial processes
- contractual arrangements with insurers preclude the disclosure of specific information
- information is protected from disclosure.
In these cases, the client and family will be informed of the reasons for restricting information.
This will be documented in the appropriate place.
Continuity of care
When a client has been harmed during care and requires further therapeutic management or rehabilitation, the client and family should be informed of their proposed ongoing clinical management. Any discharge planning should ensure that ongoing care is provided where required due to the adverse event.
Communication with the general practitioner and other CCMs
When clients leave acute care, they should ask for a discharge letter to be forwarded to their general practitioner and us. We should also be telephoned. The discharge letter should contain summary details of:
- the nature of the adverse event and the client’s continuing care and treatment
- the client’s current condition
- any clinical investigations and their results
- any relevant discharge information.
Monitoring improvements
Any changes implemented due to a review or investigation should be monitored for effectiveness. Personnel responsible for clinical risk management should develop a plan to monitor changes' implementation and effectiveness.
This information should be given to the client and family where appropriate and possible.
Communication and continued support for CCMs and staff
Effective communication with staff is vital in ensuring that recommended changes are fully implemented and monitored. It will also increase awareness of client safety and the value of open disclosure.
CCMs involved in the incident must continue to be supported to minimise residual emotional and professional harm. Continued support, including debriefing, should be active but approached with sensitivity.
Evaluation of the open disclosure process
Clients, family and other support persons should be allowed to provide feedback on the open disclosure process. The option of a face-to-face interview, where appropriate, and/or
a standardised open disclosure evaluation survey should be provided. Sensitivity around how this is conducted will be required.
Staff involved in open disclosure should also provide feedback through a standardised survey where possible. Ideally, client and staff feedback should be completed within four weeks of the end of the open disclosure process. However, sensitivity is required depending on the circumstances.
Staff involved in open disclosure should also provide feedback through a standardised survey where possible. Ideally, client and staff feedback should be completed within four weeks of the end of the open disclosure process. However, sensitivity is required depending on the circumstances.
Suggested evaluation surveys are provided with supporting materials. To access these, visit www.safetyandquality.gov.au/opendisclosure
Survey results should be regularly reported to the organisation’s management and other internal open disclosure measures.
Communication of lessons learned
We rely on internal mechanisms to communicate lessons learned and implement changes to practice as a consequence of client harm. This includes improvements to open disclosure practice based on the ongoing evaluation.
Maintaining documentation
Key considerations and actions
- Keep the client record up to date
- Maintain a record of the open disclosure process
- File documents relating to the open disclosure process in the client record
- Provide the client with documentation throughout the process.
Comprehensive documentation contributes significantly to successful open disclosure. Disclosing an adverse event and its relevant facts must be properly recorded. Recording commences at the beginning of open disclosure and continues throughout. Documentation includes client records, incident reports and records of the thorough review of the adverse event.
Documenting the open disclosure process
Documenting the open disclosure process
We require an open disclosure documentation management process in place. It is important that a record is kept of the open disclosure process, including all relevant:
- client, family and support person contact details
- all discussions
- all information provided
- logistical details, plans proposed
- agreements and commitments made.
Without breaching legal requirements, all documentation related to open disclosure should be filed in the client's record.
Key considerations for documentation
The client record must be current before the first meeting, including a comprehensive account of the adverse event as it is initially understood. In the case of death due to an incident, a copy of the client record will remain accessible to all those who will be involved in the open disclosure process.
The client record should document the following:
- time, date and place of the disclosure discussion and the names and relationships of those present
- plan for providing further information to the client and family
- offers of support and the responses received
- questions posed by the client and family and the answers given
- plans for follow-up as discussed with the client and family
- progress notes relating to the clinical situation and accurate summaries of all points explained to the client and family
- copies of letters sent to the client and family and their general practitioner.
Documentation should be made available to the client and family without breaching legal and privacy requirements. Our staff should also be aware of how to document and share information.