Managing a Urinary Catheter
How to manage a Urinary Catheter
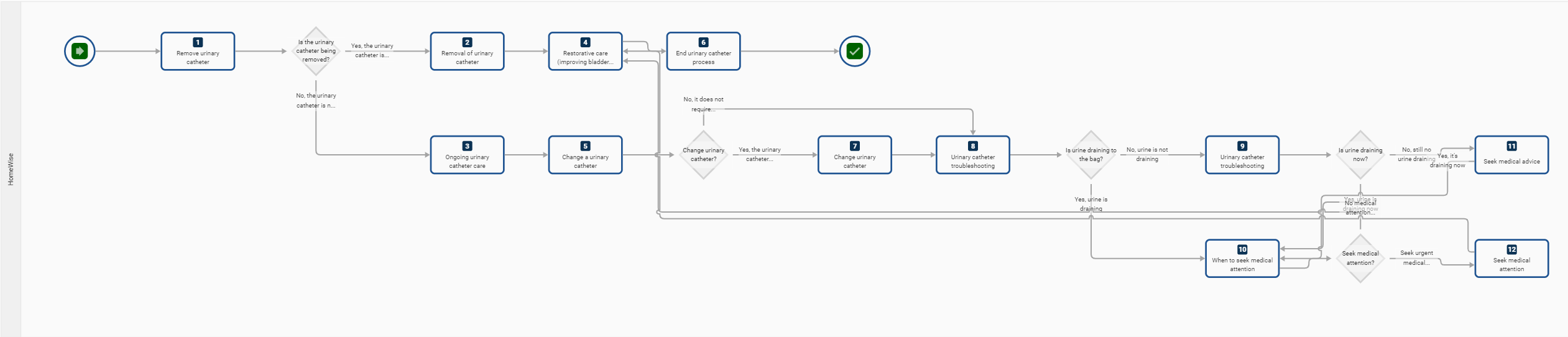
The process map below outlines the management of a urinary catheter for a client. HWH can provide some steps in this process map, and a trained catheter clinical professional can provide other steps.
HWH has the skill sets to provide steps 3, 8, 9, 10, 11, and 12. HWH staff and CCMs will escalate the remaining steps to a trained catheter clinical professional.
A process map to managing a client's urinary catheter
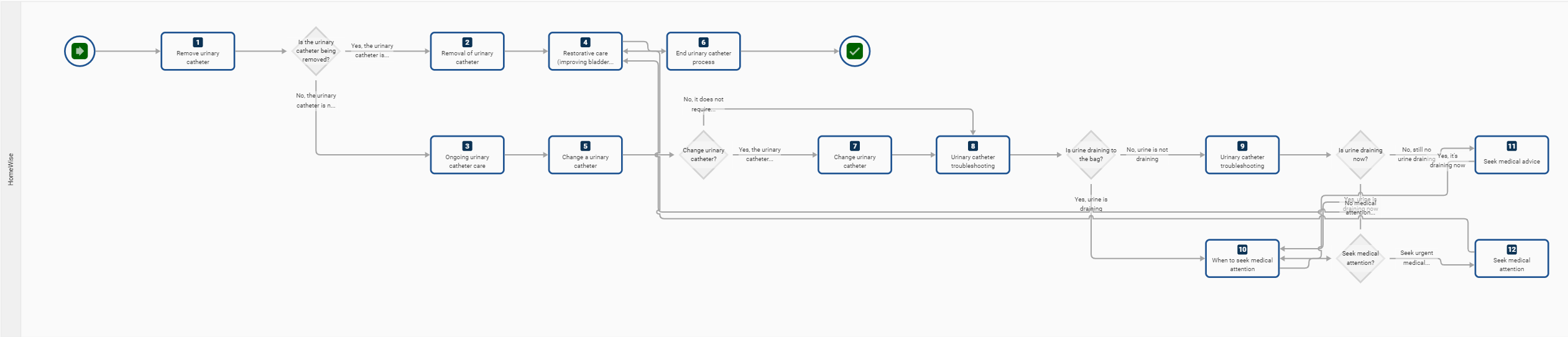
HWH has the skill sets to provide steps 3, 8, 9, 10, 11, and 12. HWH staff and CCMs will escalate the remaining steps to a trained catheter clinical professional.
A process map to managing a client's urinary catheter
{kind=link}
Related Items
- Urinary Catheter Management policy
Introduction
This process guides you when supporting a client with a urinary catheter.
This process guides you when supporting a client with a urinary catheter.
- Alterations in urinary elimination can cause anxiety and be uncomfortable and frustrating.
- Home support workers and clients must work together to promote normal urinary function.
- An essential consideration in ALL catheter care is the need for meticulous aseptic practices to prevent urinary system infection and cross-contamination.
- Staff must always be aware of signs of autonomic dysreflexia (see below), a potentially life-threatening reflex, particularly in people with spinal cord injury.
- While there are many different types of urinary catheters, this process explicitly covers three different types of catheters: indwelling, suprapubic, and in-out catheters.
Goals of Care
- promote normal micturition (urination)
- achieve complete bladder emptying
- maintain catheter drainage
- prevent infection
- maintain skin integrity
- provide a sense of comfort for clients
- Clients should be allowed the assistance of a health care professional review if needed -always escalate to the CCM, who will contact a health professional if there is any concern.
Training and Education
- All staff supporting clients with catheters must adhere to best practices in monitoring the safety and comfort of individuals who are catheterised
- All staff supporting clients with catheters must complete two Talent LMS courses -
- 5.05.0 Catheter Care Outcomes, Indicators, Policy and Processes
- 5.05.1 Catheter Management
- provide clients who need catheterisation with additional support and education
- to maintain the client's dignity and privacy at all times.
Step-by-Step Processes
Steps for supporting a client with a urinary catheter
NOTE: only trained staff can support clients with their catheter care management. HWH provides training and education on catheter care management (see above).
NOTE: only trained staff can support clients with their catheter care management. HWH provides training and education on catheter care management (see above).
1. Ongoing urinary catheter care and maintenance:
- staff need to inspect the insertion site of the urinary catheter twice a day (indwelling and suprapubic catheters)
- wash daily at the catheter insertion site. This is best done during showering (use sensitive skin body wash and avoid high pH soaps).
- All drainage bags/collection bags must be emptied at least once per shift, or every 2-3 hours, or when the bag is half full or more
- Ensure that each client has a separate sanitised receptacle for measuring urine to prevent cross-infection
- Always use hand hygiene and precautions like wearing PPE (eye goggles, apron, gloves) when emptying bags.
- Leave indwelling catheter and leg bags in situ (in original place) whilst showering the client
- workers must avoid disconnection of tubing to minimise the risk of trauma and contamination
- Ensure the collection bag is always attached to the client and is lower than the catheter to ensure adequate drainage
- Drainage equipment needs to be secured below the height of the bladder to prevent urine reflux
- Ensure the collection bag is removed only when replaced or as directed by a health professional.
Support workers can avoid exposing the client to repeated infections at the insertion site of Suprapubic Catheters (SPC) by doing the following steps to clean the insertion site at least daily:
- Prepare equipment to clean the SPC site. You will need sterile gauze pads, vials of saline solution, alcohol wipes, a sterile container, and a waste receptacle; wash your hands and don gloves.
- Clean the outside catheter tubing nearest the SPC site with alcohol wipes. Use 4 wipes and wipe away from the SPC site for up to 10 cm.
- Use a sterile container and saline-soaked gauze pads; wash around the catheter insertion site with saline solution. Use one gauze pad at a time, wipe in one direction, and then discard. Repeat at least 4 times in different directions - north, south, east, and west.
- Apply iodine solution to the cleaned area around the SPC site. Allow to air dry.
- If the client has a skin fold at the SPC site, place a sterile gauze pad near the insertion site to absorb any perspiration.
- Discard waste and wash hands.
- Do not use this process for indwelling catheters.
Watch the view to see the process for maintaining a catheter. At HWH we would use Milton sanitary solution to manage infection risks.
How to empty a catheter bag
Watch the video.
2. Diet and hygiene:
- Ensure the client drinks at least two litres of fluid (preferably water) per day
- Ensure the client eats a balanced diet (fruit, vegetables and wholemeal cereals) to prevent constipation
- After washing and showering, do not use powder, deodorant or creams around the catheter
- Urine acidity is an irritant to the skin, so keep skin moisturised around the genitalia with a barrier lotion
- good personal hygiene and soap and water are needed around the external urethral orifice to prevent infection (penis for males, vulva for females).
3. Leg drainage bags:
- If a leg bag is used, assess for tightness and impaired circulation
- If a leg bag is used, change the client’s leg bag at night before sleep; when connecting the new leg bag, be careful not to touch the end that is inserted into the catheter
- replace the old night bag with a new night bag
- note the presence of any blood clots, offensive odour, cloudy, discoloured urine
- Note any complaints of bladder spasms
- Remind clients who self-catheterise to empty every 4-6 hours and use sterile lubricant for insertion of in-out catheter.
- Ensure adequate supply and provision and store in-date stock of replacement indwelling catheters, uridomes and drainage bags, leg bags, securement devices, PPE and sterile syringes.
4. Self-catheterisation: (in-and-out catheters)
What is an in-and-out catheter?
What is an in-and-out catheter?
An IC is also known as an "in and out" catheterization. This means the catheter is inserted and left in only long enough to empty the bladder and then removed. ICs are usually done every 4 or 6 hours, depending on the person's emptying needs.
Special Note: Risks for infection are increased if:
- The staff have poor hand hygiene practices. Staff must wash hands and don gloves before touching a client's catheter.
- The connection between the catheter and the drainage bag is broken.
- The drainage device’s tap becomes contaminated when the bag is being emptied or comes into contact with the floor or an unsanitised receptacle.
- Reflux of urine from the bag into the bladder occurs because the bag is full or positioned above the bladder level.
- There needs to be better hand hygiene before the client or worker clients handling the catheter have inadequate fluid intake and/or level of personal hygiene while caring for their catheter. Clients are to drink 2 litres of water each day unless otherwise specified by the doctor.
- The catheter is inadequately secured, causing trauma to the urethra and bladder neck.
Urinary catheter troubleshooting
- No client should be denied the assistance of a healthcare professional review if needed.
- SW to escalate catheter functioning issues to the CCM or, if you are out of office hours, call HWH 24/7 on 1800 717 590.
- All staff supporting a client with a urinary catheter must be alert to potential obstruction to the flow of urine and infection risks.
- Constipation can interrupt the urine flow as the bowel presses on the catheter, resulting in urine leaking around the catheter.
- Encrustation can occur inside the catheter tube and block the flow of urine. One of the common complications of long-term catheter use is encrustation by mineral salts, leading to catheter blockage. Crystalline deposits can form on the retention balloon, obstruct the eye holes and block the urine drainage channel. If the encrustation is visible in the tube, this can be broken up at the encrustation site by rolling the tube in your fingers. If this occurs, other catheter parts may also be affected. Encrustation must be reported to the CCM and recorded in the shift notes.
- Some clients are at risk of autonomic dysreflexia if a full bladder obstructs urine flow.
Autonomic Dysreflexia
Autonomic dysreflexia is often caused by a full bladder but can also be triggered by a full bowel, bladder infection, pressure sores or tight-fitting clothes.
Call an ambulance immediately if there are signs of autonomic dysreflexia, which may include:
Call an ambulance immediately if there are signs of autonomic dysreflexia, which may include:
- high blood pressure
- sweating
- severe pounding headache
- blurred vision
- flushed face
- cool, clammy skin, goosebumps
- nausea.
What to do if a person is showing signs of autonomic dysreflexia:
- Call an ambulance
- Sit the person up
- remove tight clothing
- Check urinary catheter or tubing for kinks or clogs or an overfull leg bag
- follow urinary and/or bowel management plans.
More urinary catheter troubleshooting
If urine is not draining into the bag:
- Check if the catheter or tubing is twisted or squashed
- Check if the tubing to the bag is blocked
- Check if the leg bag is below the level of the bladder
- Check if the straps are threaded correctly and not blocking the inlet valve of the leg bag
- Swap the leg bag to another position, such as on the other leg
- Is the client constipated?
- Check if the client drinks enough fluid daily—2 litres or 8 cups, preferably water.
- Try a new leg bag.
Is urine draining now?
- No - Still no urine draining. Check the flow value is open on the catheter tube. Report to the CCM and record in shift notes. OR contact the CCM, or if you are out of office hours, call HWH 24/7 on 1800 717 590.
- Yes - The urine is draining now—record in shift notes.
When to seek medical attention
General health concerns
All staff supporting a client with a urinary catheter must know when to seek medical advice. It's essential to seek medical advice:
If there are any signs of urinary tract infection, such as:
- cloudy, bloody or smelly urine
- feeling unwell, fevers, chills or shaking
- bladder, pelvic, lower back or flank pain
- if no urine is passed within four hours
- if leakages persist
- if the catheter falls out
Urinary Tract or Bladder Infections are diagnosed through urine specimens (urinalysis). Support workers may be asked to collect urine from the catheter (Foleys) tubing or collection bag and put it in a specimen jar for laboratory pathology analysis of microorganisms where the infection is suspected. Use your PPE for the urine collection process.
Seek medical advice
- If there is still no urine draining after checking all troubleshooting points, contact the CCM, or if out of office hours, call HWH 24/7 number 1800 717 590. The client's health professional or local doctor will be contacted for treatment protocol.
- If no health professional is contactable, take the client to the nearest hospital emergency department or call an ambulance.
Restorative care
Restorative care is used to improve bladder function and is a planned process that a trained catheter clinical professional prescribes.
Restorative care is used to improve bladder function and is a planned process that a trained catheter clinical professional prescribes.
- Clients can retain/regain normal urinary function by retraining the bladder.
- This can be achieved by providing clients who need catheterisation or have been catheterised with additional support and education. This includes:
- involving the client in their care
- bladder retraining by practising a good voiding routine
- never ignoring the urge to urinate
- minimising the use of tea/coffee/alcohol (which can interfere with the way the body produces urine)
- incontinent clients need to continue the use of medication therapy like oral antiseptics or low-dose antibiotics if advised by a medical professional
- strengthening pelvic floor muscles by repeating Kegal exercises (refer to a physiotherapist
Change a urinary catheter.
A trained clinical professional completes the removal of a urinary catheter. Contact the CCM to arrange an appointment to change a client's urinary catheter.
Special Note: Catheters must not be changed by those not qualified—a disability support worker is not qualified to change a catheter but can change a drainage bag if trained.
Special Note: Catheters must not be changed by those not qualified—a disability support worker is not qualified to change a catheter but can change a drainage bag if trained.
Changing a urinary catheter is a planned process prescribed by a doctor or catheter clinician and implemented by a trained clinical professional. A client usually has a 4 - 6 week appointment scheduled for catheter changes.
The role of the support worker is always to document a catheter change in the client's shift notes and include the following information:
- The time the changed catheter was
- amount of urine collected
- colour and condition
- any leakages
A CCM (Registered Nurse) is able to change a urinary catheter. They will:
- Assemble equipment required for the change
- Change catheter following standard clinical process and aseptic techniques
- If the client self-catheterises, educate them about sterile techniques
- follow the waste management policy to discard the old catheter
- Always document catheter changes in the client's catheter management plan, including time, amount of urine collected, colour and condition.
Ending the urinary catheter process
The process ends if any of the following are true:
- The client no longer requires a catheter—a health professional removes it (workers may need to follow the restorative process step to assist a client in regaining or improving bladder function)
- The client with the catheter exits our services
- The client with the catheter passes away.
Removing a urinary catheter (is always completed by a trained clinical professional).
As a guideline:
- The decision and timing of when to remove a catheter needs to be made by a health professional
- The client will require monitoring and follow-up care to ensure a return to a regular voiding pattern
- Use a bladder ultrasound scanner to measure residual urine volume within 8 hours of indwelling catheter removal
- Failure to void or urinary retention are severe issues, and the bladder will require draining as soon as possible
- If the client experiences urinary continence, a continence assessment may be required
- Monitor for any signs of fever, confusion, pain, or bleeding and exclude urinary tract infection
- Dispose of catheters and drainage bags as per waste/disposal policy to prevent cross-contamination.