Introduction This policy is about regulated restrictive practices. A restrictive practice is defined as any practice or intervention that restricts the rights or freedom of movement of a person, with the primary purpose of protecting the person or others from harm.
Prohibited Practices Any practice or action that may be experienced by a person as noxious, unpleasant or painful. Types of prohibited practices include aversive, consequence-driven, exclusion, and psychosocial restraints.
Prohibited practices include but are not limited to:
any form of corporal punishment (for example, smacking or hitting)
any punishment intended to humiliate or frighten a person
any punishment that involves immobilising a person with chemical or physical restraint, including supine and prone restraint holds
force-feeding or depriving a person of food
use of medication to control or restrain a person without a behaviour support plan, proper medical authorisation or legal consent
use of punishing techniques, such as putting a person in a hot or cold bath, putting spice in their food, or squirting the liquid on their face or body
overcorrection, where the punishment is out of proportion to the behaviour (for example, making a person clean an entire room because they tipped their meal on the floor)
confinement or containment of a child or young person (anyone under 18 years of age), such as forcing them to remain in a locked room or other places that they can’t leave
punishment that involves threats to withhold family contact or change any part of a person’s lifestyle plan
denying access to basic needs or supports
unethical practices, such as rewarding a person with cigarettes or alcohol
any other act or failure to act that is an offence under federal, state or territory laws.
Prohibited practices are practices that must never be used. They may unlawful or unethical. Any prohibited practice may be a criminal offence or civil wrongdoing. Any use of a prohibited practice is a reportable incident under the NDIS (Incident Management and Reportable Incidents) Rules 2018 (Cth).
Regulated Restrictive Practices Only regulated restrictive practices are allowed and then only with strict controls. Regulated restrictive practices include:
Chemical Restraint
The use of medication or chemical substances for the primary purpose of influencing a person’s behaviour or movement. It does not include the use of medication prescribed by a medical practitioner for treating a diagnosed mental illness or physical condition.
Environmental Restraints
Any restriction to a person’s free access to all parts of their environment. For example:
locking cupboards and refrigerators
taking away things people like
stopping the person from going to places they enjoy.
Mechanical Restraint
The use of a device to prevent, restrict or subdue a person’s movement for the primary purpose of influencing their behaviour. It does not include the use of devices for therapeutic or non-behavioural purposes. For example, it may include using a device to assist a person with functional activities as part of occupational therapy or to allow for safe transportation.
Physical Restraint
The sustained or prolonged use or action of physical force to prevent, restrict or subdue movement of a person’s body, or part of their body, for the primary purpose of influencing a person’s behaviour.
Seclusion
Sole confinement of a person in a room or physical space at any hour of the day or night where the voluntary exit is prevented, impeded or not facilitated.
Applies
to all services provided to HWH clients with a positive behaviour support plan that includes the use of a regulated restrictive practice
when a prohibited practice or unauthorised regulated practice is used
to all HWH representatives, including key managers and home support workers
Related Items
NDIS (Quality Indicators) Guidelines 2018 (Cth)
NDIS (Restrictive Practices and Behaviour Support) Rules 2018 (Cth)
Regulated restrictive practices with children and young people - Practice Guide
We support the reduction and elimination of the use of restrictive practices. Any use of restrictive practice will consider the client's cultural and communicative needs. We will only use restrictive practices:
as a last resort, and with proof, all other ways of evidence-based, person-centred and proactive strategies have been tried first
if the behaviour might harm the person or others
for the shortest time possible
in the least restrictive way possible
that is proportionate and justified
if the client or the client’s guardian has given consent
if the appropriate authorisation by state or territory bodies has been granted
if we have first understood why the client has complex behaviour and how the restrictive practice will affect the rights of the participant
if the practice is written in an NDIS lodged positive behaviour support plan developed by a positive behaviour practitioner or specialist in consultation with the client, the client’s family, support network and/or advocate.
We will be transparent and accountable for using restrictive practices through accurate record-keeping and reporting.
We will regularly review records to assess the success, need and application of restrictive practices.
Impact of Restrictive Practices
Research has demonstrated that restrictive practices do not effectively address underlying behavioural functions nor modify persistent concerning behaviour.
Research has also demonstrated that routine and ongoing restrictive practices on clients, client support networks and workers can be profoundly negative.
The use of the restrictive practice, whether on a single or ongoing occasion, according to the NDIS Quality and Safeguards Commission, can result in:
participants feeling a loss of dignity
reduced interpersonal relationships between participants and others
limited freedom and potential human rights violations
medication dependency
physiological and neurological changes
increased mental health illnesses
trauma and psychological distress, including post-traumatic stress disorder (PTSD) for participants, workers and support networks
secondary forms of concerning behaviours in response to the use of restrictive practices.
With this knowledge and understanding, we continuously monitor, evaluate and seek to reduce the use of restrictive practices with the goal of total restrictive practice use elimination.
Reduction and Elimination
We are committed to the reduction and elimination of restrictive practices and upholding the human rights of people with disability in line with the UN Convention on the Rights of Persons with Disabilities, NDIS Safeguarding Framework and the National Framework for Reducing and Eliminating the Use of Restrictive Practices in the Disability Service Sector.
We are committed to achieving this by following the core strategies:
Person-Centred Focus
Including the perspectives and experiences of people with disability and their families, carers, guardians and advocates during restrictive practice incident debriefing, individualised positive behaviour support planning, staff education and training, and policy and practice development.
Leadership Towards Organisational Change
Making the goal of reducing restrictive practices a high priority and providing support to staff to achieve it.
Use of Data to Inform Practice
Mechanisms such as periodic review of positive behaviour support plans containing a restrictive practice, provider reporting on the use of restrictive practices, reporting client assessments and individual/positive behaviour support plans—should be used to assess whether restrictive practices are still needed and consider possible alternatives. Data is also vital to determine what factors effectively reduce or eliminate the use of restrictive practices, as well as highlight areas for workforce training and development.
Workforce Development
Essential needs include understanding positive behaviour support and functional behaviour assessment, skills for trauma-informed practice, risk assessment, de-escalation, and alternatives to restrictive practices.
Use Within Disability Services of Restraint and Seclusion Reduction Tools
Use evidence-based assessment tools, emergency management plans and other strategies integrated into each individual’s positive behaviour support plan. Changes to the therapeutic environment. Meaningful activities aimed at lifestyle improvement and increased engagement.
Debriefing and Practice Review
Regular reviews of the use of restrictive practices to identify areas for practice and systemic improvement. Suppose an unanticipated or emergency use of a restrictive practice occurs. In that case, an immediate debriefing should occur to ensure that everyone is safe, that satisfactory information is available to inform later structured debriefing, and that the client is safe and being appropriately monitored.
Client Assessment
We will assist in identifying clients with complex behaviour support needs and refer them to an NDIS-approved positive behaviour support client for assessment.
A positive behaviour support practitioner, in consultation with the client, client's family, support network and/or advocate and the organisation, will be responsible for establishing a positive behaviour support plan which may include restrictive practices.
Restrictive practices in a client's positive behaviour support plan will have clear protocols for implementation and use. These practices will be reviewed at least every 12 months to reduce or eliminate the requirement of restrictive practices.
Authorising restrictive practice Commonwealth, state and territory legislative and policy frameworks provide guidelines around the use of restrictive practices, including that the intervention is the least restrictive response available, is used only as a last resort, that the risk posed by the proposed intervention is in proportion to the risk of harm posed by the behaviour of concern and with the intent to reduce and eliminate the use of the restrictive practice.
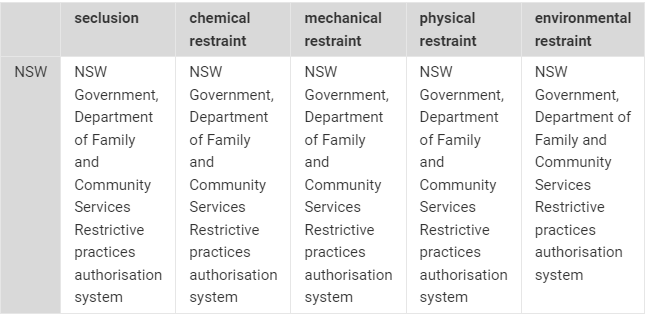
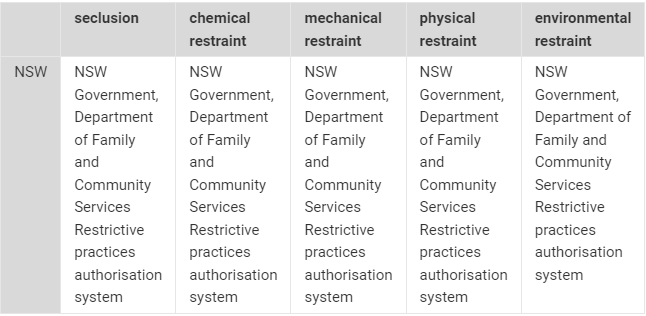
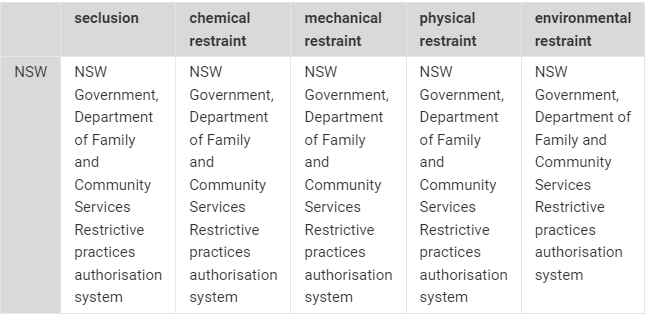
The use of a restrictive practice will only be approved as part of a positive behaviour support plan. Clients or the client's guardian, the person responsible or substitute decision-maker, must consent to the proposed restrictive practices included in the positive behaviour support plan. We must also have the relevant state or territory approval to implement and use restrictive practices. The relevant approving authorities are detailed below.
image.png
Download Record keeping We will keep a record of the following:
restrictive practices that are ongoing (e.g. chemical restraint with a daily fixed dose)
restrictive practices that are ‘unscheduled’ (e.g. physical restraint, seclusion, chemical restraint prescribed on an ‘as-needed basis, also known as PRN medication)
occasions when the use of an unauthorised restrictive practice is defined as a serious incident—also reported as a serious incident.
The detail of the report on the use of regulated restrictive practices includes:
a description which includes:
the impact on the client or others
any injury to the clients or others
whether the use was a reportable incident
why it was used
a description of the behaviour of the client that leads to its use
the time, date and place at which its use started and ended
the names and contact details of the persons involved in its use
the names and contact details of any witnesses to its use
the actions are taken in response to its use
what other less restrictive options were considered or used before
the actions taken leading up to its use, including any strategies used to prevent the need for the use of the practice.
All records must be kept for at least 7 years from the date of the document.
Reporting Authorised Restrictive Practices to the NDIS If we support clients with positive behaviour support plans that include the routine use of a regulated restrictive practice, we will report on the use of those practices each month to the NDIS Commission. This report will include:
type of restrictive practice used
a brief description of the practice
details of medication (if required)
related behaviour concern.
If we support clients with positive behaviour support plans that include as-needed use (PRN) of a regulated restrictive practice, we will report on the use of those practices each month to the NDIS Commission. This report will include:
type of restrictive practice used
a brief description of the practice
details of medication (if required)
related behaviour concern
date used
time commenced
time ceased
our incident report reference.
If we support clients with positive behaviour support plans that include a regulated restrictive practice, but the practice was not used during the reporting month, we will submit a NIL report to the NDIS Commission.
Suppose we support clients with short-term approval from a state or territory on using a regulated restrictive practice. In that case, we will report to the Commissioner every 2 weeks on using those regulated restrictive practices while the approval is in force.
Supporting Clients When a Restrictive Practice has Been Used
If a restrictive practice is used, clients and workers will be immediately supported to manage the impact of the use of restrictive practices.
If the incident is deemed reportable, a participant should be immediately referred to and assessed by a medical practitioner (where appropriate). The immediate procedure following a restrictive practice for a client must be detailed in the client's behaviour support plan and in the incident report submitted to the NDIS Commission.
Clients, and with their consent, their support network should be included in the review of their support plan following the use of any restrictive practice.
Unauthorised Use of Restrictive Practices
Unauthorised use of restrictive practices is an instance of use:
without a positive behaviour support plan and not compliant with state or territory legislation (during transitional stages of the NDIS)
without the proper authorisation
without knowing that something is a restrictive practice
for too long and without regular review
for reasons other than keeping people safe
to control a person or to make a person act in a certain way
as a form of abuse and neglect
due to a lack of training, knowledge or reflection about less restrictive alternatives.
If we have instigated any form of unauthorised restrictive practices described above, we must:
report the incident to the NDIS Quality and Safeguards Commission within five business days or 24 hours if the incident harmed the participant
report the incident to any state or territory as required.
If the regulated restrictive practice is ongoing, then we will:
obtain authorisation (however described) for the ongoing use of the regulated restrictive practice from the relevant state or territory as soon as reasonably practicable
lodge evidence of that authorisation with the NDIS Commissioner as soon as reasonably practicable after it is received
arrange the development of an interim behaviour support plan for the participant by a specialist behaviour support provider that covers the use of the practice within one month after its first use
arrange the development of a comprehensive behaviour support plan for the participant by a specialist behaviour support provider that covers the use of the practice within 6 months after its first use.
Training and Worker Requirements
The use of restrictive practices poses a serious risk due to the significant and severe impact they have on clients, their support networks, and workers.
To mitigate the risks, workers who support clients with a positive behaviour support plan (PBSP) that includes restrictive practices will be trained and at a minimum, understand:
what a restrictive practice is
what an authorised and unauthorised regulated restrictive practice is, including when, why and how they are to be used according to the positive behaviour support plan
their obligations to safely and effectively implement plans
the reporting obligations defined in the NDIS (Incident Management and Reportable Incidents) Rules 2018 (Cth)
the ethical and safety obligations following the use of restrictive practices, including medical assessments, psychological assistance and debriefing
this policy.
Workers who implement restrictive practices will work collaboratively with the behaviour support practitioner who developed the PBSP plan and all relevant allied health workers to ensure the safest and most effective plan is implemented.
All training will be recorded on our Staff training and development register and periodically reviewed to ensure up-to-date knowledge and practices.
Breach of Policy A breach of this policy may place the organisation in breach of NDIS Guidelines, which could result in:
an investigation into the organisation by the NDIS
the organisation being de-registered from the NDIS
civil penalties
criminal convictions and fines.
Any employee who breaches this policy will face disciplinary action up to termination of employment.
{kind=link}