Seizures Management
What is it?
A seizure occurs when abnormal electrical discharges and neuronal activity cause a brain disturbance. An individual will then be diagnosed with epilepsy if they have had two or more unprovoked seizures that are not known to cause a medical condition (Epilepsy Foundation 2014).
Types of Seizures
There are two major groups of seizures: primary generalised seizures and focal or partial seizures. Primary generalised seizures involve both hemispheres of the brain at once. In contrast, focal seizures involve electrical disturbances in one specific brain area, which may then spread to other brain areas. Partial seizures are generally a result of head injuries, infection, stroke, or tumours, whereas primary generalised seizure causes often involve hereditary factors (Epilepsy Foundation 2013).
Focal (Partial) Seizures
Focal seizures can present in people as unusual behaviours and may appear as the person simply daydreaming. There are three types of focal seizures including:
Focal seizures can present in people as unusual behaviours and may appear as the person simply daydreaming. There are three types of focal seizures including:
- Focal seizure – awareness is retained, formally known as ‘simple partial seizures
- Focal dyscognitive seizure – awareness is altered, formally known as ‘complex partial seizures
- Focal seizures evolving to bilateral convulsive seizure
(Epilepsy Action Australia 2016)
Generalised Seizures
Because generalised seizures result from abnormal electrical activity in both hemispheres of the brain, the individual will generally lose consciousness at the onset of the seizure (Epilepsy Action Australia 2016). Types of generalised seizures include:
-
Absence:
- Typical: Patients will stop what they are doing and lose consciousness of the event; they will appear to have a glazed or vacant look on their faces and are unaware of their surroundings. These seizures will generally last for ten seconds and stop abruptly.
- Atypical absence: Sometimes, during these seizures, the patient’s loss of awareness is incomplete. These seizures will often last longer than a typical absent seizure, and the patient will have a longer recovery time.
- The absence with special features.
-
Myoclonic absence: When patients experience a brief contraction of a muscle, muscle group or several muscle groups caused by the cortical discharge. They generally last for a short time only (less than five seconds) however, they can lead to a generalised tonic-clonic seizure.
- Clonic: Patients will experience asymmetrical jerking without any prior stiffening.
- Tonic: Patients will experience a sudden increase in muscle tone, which contracts their muscles. This results in their neck extending, hands clenched in a fist or flexed open, facial muscles contract opening, the eyes and arms contract, and the patient's legs extend out, causing them to fall if standing. These seizures are brief, and some patients will regain consciousness before they hit the floor.
- Tonic-Clonic: This type of seizure was previously known as a ‘grand mal seizure’ and is often the type of seizure most commonly envisioned. This type of seizure consists of both a tonic and clonic stage (described above). Movements characteristic of the tonic phase will occur and continue for up to thirty seconds before the seizure continues into the clonic phase. During the clonic phase, the individual will experience convulsive movements, impaired breathing, excessive salivation and changes in some autonomic functions. Following this, the patient may regain consciousness slowly but may remain confused and sleep deeply.
- Atonic: Patients will experience a sudden loss of tone in their postural muscles, and consciousness will be lost for a split second. If the patient is standing, they will fall. however, there is a quick recovery time, and most patients can stand up straight away.
- Myoclonic: Sporadic jerks will be experienced by the patient, usually bilaterally.
Nursing Management of Someone Having a Seizure
Patient safety is one of the main considerations during seizure activity; it is important to remember DRSABCD:
- Danger
- Response
- Send for help
- Airway
- Breathing
- Circulation
- Defibrillation
The nurse must stay with the patient and call for help. It is essential to note the time the seizure started and its characteristics. Protection must be given to the patient’s head, especially with any convulsive movements that may injure the patient. The surrounding area must be made clear to decrease the risk of injury; however, it is essential not to try to physically restrict the movement of the patient’s limbs as this can cause musculoskeletal damage. You can protect the patient from harming themselves by using pillows and bed rails if needed.
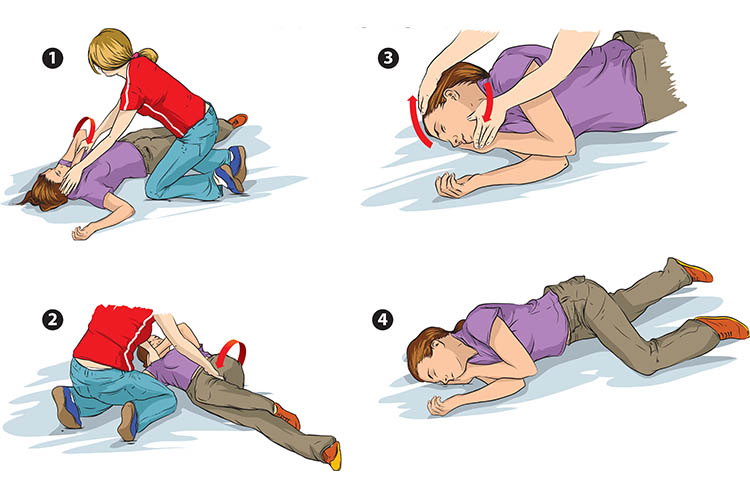
Attempts can be made to turn the patient into a recovery position. If this is not possible, it is essential to be done when the patient’s limbs relax, to prevent aspiration due to excessive saliva production, and to ensure their airway remains patent. Suction and oxygen must be available, and if possible, a soft oral airway can be placed, providing you don’t have to force teeth apart to place it. Monitoring of vital signs is imperative, especially respiratory function.
Following the seizure, monitoring the patient’s airway, using suction as needed, and allowing the patient to sleep is important. When they wake, they may need to be informed of what has occurred and reassurance given, as this can be distressing for the patient.
Frequent monitoring of vital signs and neurological observations will need to be done on the patient to monitor their condition.
Note:
Medical conditions MUST always be diagnosed by a medical professional.
The above has been structured to provide basic information to HWH Support Workers and Clinical Care Managers.