Enteral feeding is the delivery of a nutritionally complete feed containing protein, carbohydrate, fat, water minerals and vitamins into the stomach, duodenum or jejunum.
Decisions on tube route, content and nutritional management are best made by the client’s multidisciplinary care team and put into place only by skilled medical professionals with consent from the client, their family, carer, and/or guardian.
Procedures for administering enteral feeding should be outlined in a standard protocol available from health care personnel.
Delivery options include continuous infusion by pump, intermittent by gravity, intermittent bolus by syringe and cyclic feeding by infusion pump. Individuals of any age may require tube feeding so care should be tailored according to the client (e.g. infant or adult).
Paediatric enteral feeding/nutritional support requirements can differ from adult needs. The clinical indications for children requiring enteral feeding can include but are not limited to cerebral palsy, premature infants, ventilated clients and those who suffer cancer, cystic fibrosis, or Crohn's disease.
Children will need special infant formulas and high-energy feeds in order to cater adequately for their particular growth and nutritional needs.
Who Has an Enteral Tube?
Enteral tube feeding is usually considered for a person who is malnourished or at risk of malnutrition and has:
an inadequate or unsafe oral intake and
a functional, accessible gastrointestinal tract.
This can be due to a range of conditions:
anomalies of the throat, oesophagus or bowel
anorexia
impaired swallowing capacity
orofacial deformities/fractures
neurological or psychiatric conditions
severe debilitation
respiratory distress.
Responsibilities
NOTE: It is VITAL that only skilled and trained personnel manage and care for those who require enteral tube feeding.
HWH's key managers must ensure that care workers can set up pump feeds and administer bolus feeds correctly.
Failure to do so may result in the incorrect volume of feed being delivered and microbial contamination of feed. CCMs must identify workers who require training and organise specialised education accordingly.
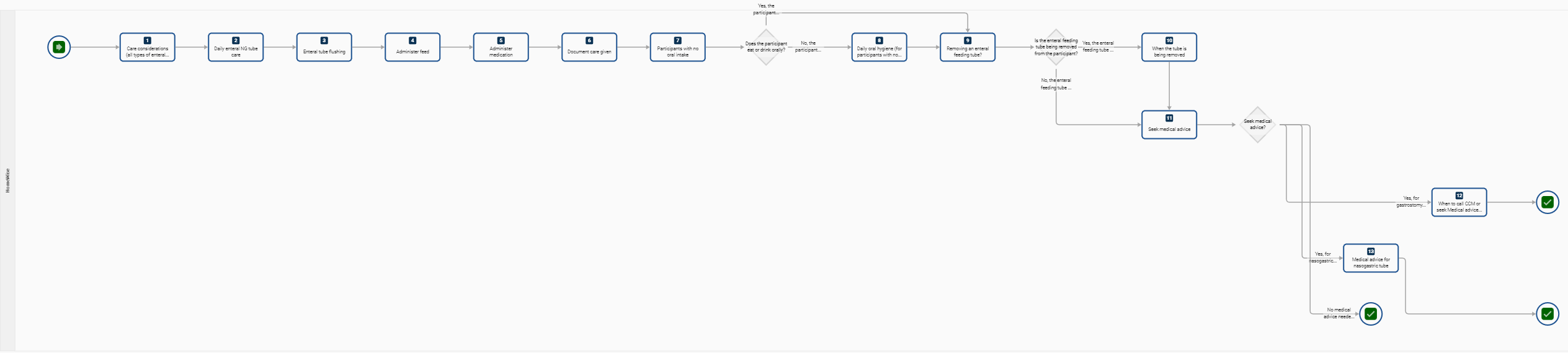
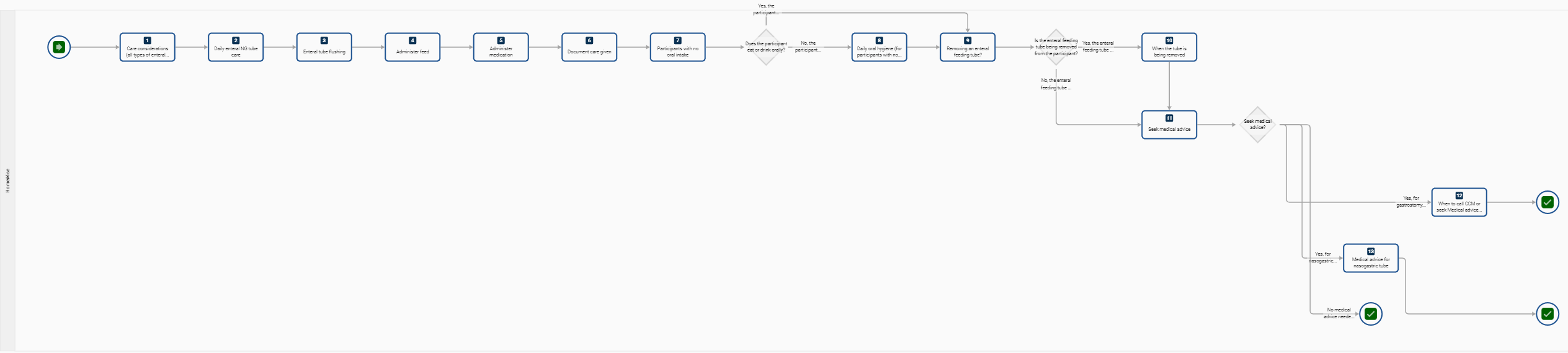
Step 1 - Care Considerations
Care considerations for all types of enteral tube feeding:
If the client is confused/disoriented or physically restless, get help from another worker
Clients with enteral feeds may experience disturbed body image and require positive reassurance and support of family members and friends
Insertion Site
Assess insertion site every shift, assess skin condition and check for abnormalities
Monitor drainage or leaking of gastric contents
Apply gauze dressing if there is drainage (if the dressing is used, change it as required)
Gently rotate the tube 360 degrees (unless advised otherwise by a medical specialist).
Remember that clients need water which may be administered by bolus
Tubing and Tape
Beware of an allergy to tape used for anchoring tubing—record and document as required.
Check tube is anchored, looped and securely taped (should not be hanging freely)
Check tube length using the tube markers to ensure the tube is in the correct position and not displaced
Step 2 - Daily enteral NG tube care
Daily care for a person with NG tube:
maintain hand hygiene and wear disposable gloves
Provide privacy for the client
inspect the condition of nostrils and, oral cavity, mucosa and note down
Elevate the head to 30 degrees
Checking the length of tubing is recommended once per shift to reduce the risk of aspiration due to tube migration
Clamp tubing when not being used
PEG Stoma Care and Advancing the Tube
The PEG stoma site will require cleaning each day. The feeding connector requires rotating once a day.
Stoma Cleaning Equipment:
PPE - gloves
A small bowl of cool boiled water
Soft gauze swabs
Alcohol wipes
A bowl to discard used swabs and alcohol wipes
Stoma Cleaning and Rotating the Feeding Tube:
Hand Hygiene and PPE
Use cold boiled water and soft gauze to clean the stoma site, wash all around the stoma site and surrounding area, and clean in one direction only - clockwise.
Discard the used swabs in a bowl.
Rotate the tube once a day - one turn in a clockwise direction so the tube moves freely.
Advancing the Feeding Tube
PPE - change gloves
Sanitise the first 10 cms of the feeding with an alcohol wipe.
Undo the tube clip
Advance the feeding tube into the stoma (5 cms) and return to the usual position.
never advance tubing where there is resistance
Leave a finger-wide space between the stoma and the tube clip and secure the tube clip.
Syringe Cleaning Method:
Pull apart the plunger from the barrel
Place the plunger and the barrel in a bowl with mild detergent and wash by shaking the water through the syringe parts, replace plunger into the barrel and draw soapy water into the syringe and push through syringe Luer lock to clean.
Repeat step 2 in cool boiled water to rinse syringe barrel and plunger
Allow to air dry on a paper towel
Store clean syringe parts in a clean airtight container.
Step 3 - Enteral Tube Flushing
Flush Equipment
Hand Hygiene - PPE
60 ml syringe
Jug of cool boiled water
A clean container
Flush Method
Draw up 60 mls cool boiled water in the syringe and place in a clean container
Remove feeding tube from Statlock or Hyperfix in position
Close the clamp on the feeding tube
Remove the stopper from the feeding port
Push a syringe of water into the feeding tube port and twist
Open the clamp on the feeding tube
Flush the water into the feeding tube using a push-pause technique
Close the tube clamp on the feeding tube
Remove the syringe from the port
replace stopper on feeding port
Replace tube on to Statlock or Hyperfix in position
Step 4 - Administer feed
Equipment
Hand Hygiene - PPE
60 ml syringe
Jug of cool boiled water
A clean container
specifically prepared and measured food or feed according to the client's needs
giving set if required
Guidelines
Prime feeding tube with 100 mls of cool boiled water before food administration
Foods are to be given through the feeding port of the feeding tube
Foods should be in liquid form
Flush the feeding tube after feeding. Use a 60ml syringe with 30mls of water (every 4-6 hours for continuous feeds)
Infection control: wipe the top of the formula with an alcohol swab before opening—No feed should be hung for more than 8 hours—do not add a new formula to the old
dispose of used materials correctly to prevent the spread of microorganisms
positioning of the syringe prevents the introduction of air into the tubing
never force solutions
If feeding intermittently, feed volume is usually 200-500 mls per feed
If you have any concerns about feeding progress, cease administration by TURNING OFF the infusion pump or clamping or kinking the feeding tube.
To administer foods
Hand hygiene and PPE
Firstly, ensure the feeding tube has been flushed
Close the tube clamp on the feeding tube
Ensure the person is positioned at 30 degrees for feeding
Check that the feeding tube is positioned correctly and not kinked
Check the expiry date of the feed/shake bag or bottle
Measure liquified prepared food and draw it up into a syringe OR select purchased prepared food container
Remove the stopper from the feeding port
Push the syringe into the feeding tube port and twist to secure Luer lock OR use an aseptic technique and hang the bag on a drip stand and prime giving set or with a bolus, connect the syringe to a feeding tube.
Open the tube clamp.
Administer the food using a push-pause technique on the syringe plunger OR connect the giving set to the feeding tube and set the feeding rate on the pump or use gravity to allow the feed to flow
To complete the feed flush the feeding tube with 100 mls cool boiled water
Close the port and close the tube clamp
Replace tube onto Statlock or Hyperfix in position
monitor for mishaps, i.e. allergy, reflux, diarrhoea and maintain physical comfort
record details.
Step 5 - Administer medication
Equipment:
Hand Hygiene - PPE
60 ml syringe
Jug of cool boiled water
Tablet crusher
Medications
Medication cup
Spoon
A clean container
Guidelines:
If in any doubt about efficacy and administration, consult and confirm with the pharmacist
Liquid medication or soluble tablets are advised
mortar and pestle can be used to crush some tablets
Give each medication separately and make sure the tubing has been flushed of residue before and after dispensing
monitor for any adverse reaction to the new medication.
To administer medications -
Hand hygiene and PPE
Firstly, ensure the medication tube has been flushed
Close the tube clamp on the feeding tube
check medication order
Measure liquid medications into a medicine cup and dilute with cool boiled water OR Crush tablets with a pill crusher and mix with 20ml cool boiled water.
Draw up the diluted medication in the syringe
Remove the stopper from the medication port
Push the syringe into the medication tube port and twist
Open the tube clamp
Flush the water into the medication tube using a push-pause technique
If more water is required to flush the tube repeat the procedure
Close the port and close the tube clamp
Replace tube onto Statlock or Hyperfix in position
Repeat the steps for each medication and remember to administer each medication separately.
Step 6 - Document care given
Keeping good records is advised to maintain quality care for those dependent on enteral feeding.
Shift notes are important to track what, when and how care has been given.
A client checklist might include details such as
date of insertion
Skin condition around the access site
Client age, medical history/physiological state
weight and body mass index
nutritional goals and hydration needs
date of dietician/clinical review
type of feed, equipment and tube gauge in use
daily monitoring essentials
fluid balance chart and bowel movement chart
emergency actions, contact phone numbers for family, doctor, and hospital.
Please report any concerns to the relevant CCM
Step 7 - Clients with no oral intake
Oral hygiene is important for all clients, even without oral intake.
Decision A - Does the client eat or drink orally?
No - Step 8 -
Yes - Step 9 -
Step 8 - Daily oral hygiene (for clients with no oral intake)
Oral hygiene is still important for clients who receive all nutrition and fluid needs via enteral tube feeding. Daily oral hygiene includes:
gentle brushing of teeth, gums, tongue and palate with a soft toothbrush and mild toothpaste (suction devices and suction toothbrushes may be necessary for some participants with difficulty swallowing)
mouthwash (if recommended by a medical specialist) taking care to avoid aspiration. May require a specific non-alcoholic mouthwash to avoid drying out.
Maintain moisture in the mouth if required with swabs and lip moisturiser
Step 9 - Remove an enteral feeding tube.
A qualified health professional decides when to remove an enteral feeding tube.
Decision B - Is the eternal feeding tube being removed from the client
Yes - Step 10
No - Step 11
Step 10 - When the tube is being removed
Regarding tube removal:
When to remove a feeding tube is decided by a qualified health professional
If a balloon held gastrostomy tube has been pulled out or has fallen out it needs to be replaced by a competent worker before the stoma closes
Always verify the order to discontinue tube feeding
Paediatric removal might require sedation of an individual in the hospital
Only a clinical nurse or other health professionals can remove a feeding tube.
Consent should be obtained before the removal of the tube
Care workers need knowledge of the risks and complications of removing enteral feeding tubes
escalate care as appropriate.
Step 11 - Seek medical advice
When to seek medical advice can differ between individuals and the type of enteral tube being used.
Decision C - Do you need to seek medical advice
Yes - for gastronomy tube or device (PEG) - Step 12
Yes - for nasogastric tube (NGT) - Step 13
No - Step 12
Step 12 - When to call or seek Medical advice for gastronomy tube or device This applies to clients with a gastrostomy tube or device only (e.g. PEG).
Inadvertent removal of the tube
If the stoma is immature (less than 6 weeks), the stoma will close within 2-4 hours. If this happens, a new procedure would be required. Call an ambulance or take the person to the nearest emergency department immediately.
If the stoma is mature (6 weeks or more):
contact the client's medical specialist, local gastroenterology unit or emergency department
The client may require an immediate radiology contrast study/endoscopy procedure to reposition the tube
Other potential gastrostomy feeding problems
When to call the CCM:
If there is hyper granulation of the stoma site
excoriation or breakdown of skin around the access site
infection—monitor for fever, redness greater than 1 cm around the insertion site or swelling
nausea, vomiting or regurgitation—this might indicate improper placement of tube or aspiration into the lungs
respiratory difficulty
a sore throat or irritated pharynx
abdominal pain or distention, diarrhoea or constipation
signs of malnutrition, organise fluid and electrolyte pathology testing.
There is drainage or leaking of gastric fluid or contents or tube feed
the tube becomes displaced.
Step 13 - Medical advice for nasogastric tube
Seek medical advice when supporting a person with a nasogastric tube if:
There is redness and swelling around both nostrils
The tube is blocked, and you can’t unblock it
The patient gags. Check the pharynx with a torch and tongue blade
there it is suspected that the tube has moved, e.g. poor tolerance to feed, reflux of feed into the throat, discomfort in the throat, change in tube length is suspected
The tube falls out, and you are unable to replace it
The tube needs to be replaced
If you have any concerns about feeding progress, cease administration by TURNING OFF the infusion pump or clamping or kinking the feeding tube.
{kind=link}