Complex Wound Management
Guidelines for managing complex wounds
Overview
Introduction
- When supporting clients with complex wounds, it’s important to provide consistent individualised support as there are physical, psychological and social impacts of living with a wound.
- Wounds can cause pain, systemic illness, increased time in hospital, extended absence from normal activities, low self-esteem and altered body image.
- A person’s wounds can be interfered with and/or affected by:
- medication—drugs that suppress the immune system or thin the blood
- age—being elderly means the risk of infection is higher, scar tissue is more fragile and other health conditions are more likely
- smoking (including passive smoking)—increased risk of infection, dampened inflammatory response and hypoxia (deficiency in the amount of oxygen reaching the tissues)
- decreased mobility/lack of exercise—particularly a lack of ankle mobility can result in lower limb oedema or venous congestion and ulceration
- obesity—increases the risk of wound dehiscence and infection and venous hypertension
- inappropriate dressings—adherent dressings can cause damage while other dressings stay too wet or interfere in other ways
- rough handling of the wound—new granulation or epithelium may be damaged
- poor general health—other health conditions can cause hypoxia or impede or delay healing.
- Wound healing can be complex and is affected by numerous general and local factors. With this in mind, it is important to support the whole person and not just treat the wound.
Palliative care
- Where palliative care is being provided, healing is not the primary aim.
- The goal, then, is to ensure comfort and freedom from pain, itch, malodour and haemorrhage.
Wound assessment
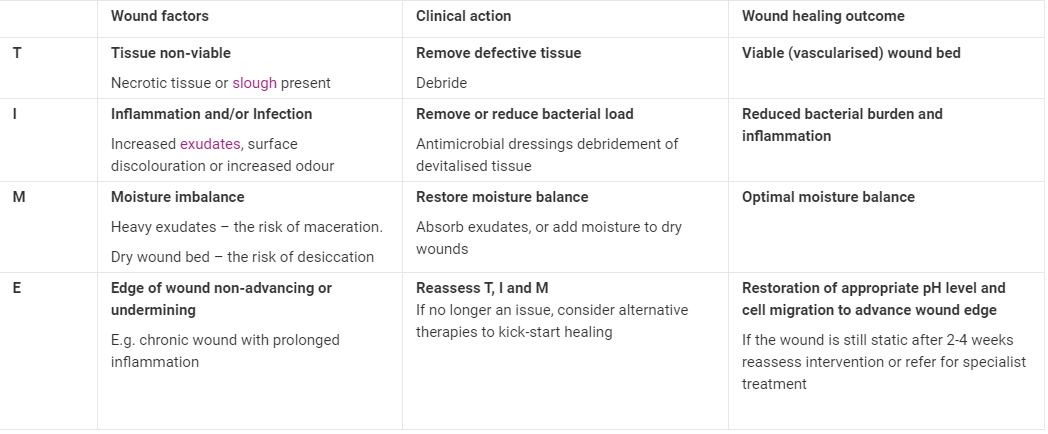
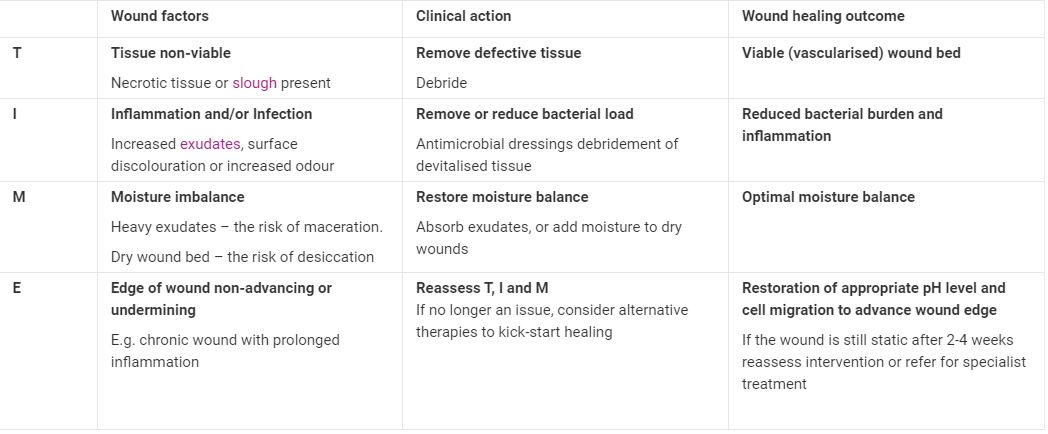
- Wounds should be assessed for any local barriers to healing, and the results should be documented at each dressing change using the following TIME assessment tool.
- The TIME abbreviation is a summary of the principles of wound bed preparation.
- It can be used as a memory aid to guide practice, heal wounds quickly and help clients have a more comfortable path to healing.
{kind=link}
Wound cleansing
The aim of wound cleansing is to remove gross contamination with minimal pain to the person and minimal trauma to the tissue. Wounds should be cleaned to:
- remove excess exudates
- remove slough and/or necrotic tissue
- remove remnants of previous dressings
- facilitate accurate assessment of the wound/wound bed
- promote patient comfort.
Wound infection
- Recognising the distinction between contamination, colonisation and infection is important when supporting a client with complex wounds.
- Contamination occurs when small numbers of bacteria are detected in a wound, but their presence is short-lived and they do not multiply.
- In a colonised wound, bacteria not only increase but become established. Once an infected wound passes critical colonisation, it may start to affect wound healing.
Wound dressing
- A moist environment at the wound/dressing interface should be selected when selecting dressings. The wound dressing product should be appropriate to meet the needs of the wound and/or promote the next stage of the wound-healing matrix, taking into account TIME.
- In wound care, accurate pain assessment is essential for choosing the most appropriate dressing.
- Pain assessment before, during and after the dressing change can provide vital information for future wound management.
- An exception is a person with peripheral neuropathy who may have lost sensation and therefore not able to feel pain e.g. diabetic patients may be unable to feel pain in the foot.
- In general, pain experienced by a person, although subjective and variable from person to person, falls into the following categories:
- a deep, dull, constant pain
- a superficial burning type of pain
- a neuralgic type of pain
- an ischaemic type of pain
- pain resulting from cellulitis.
- Whatever the cause of the pain, the person’s perception should be acknowledged, and appropriate action should be taken to alleviate the pain.
- The wound dressing should be appropriate to the wound's type, location and size.
- Any wound dressing with leakage or strikethrough that breaks the barrier it provides against external contamination should be changed.
- If changing the dressing in a timely manner is not possible, apply a dressing pad over the area of the strikethrough to establish appropriate physical barriers.
- If leakage or strikethrough occurs frequently, it may be appropriate to re-evaluate the dressing product choice.
- The effectiveness of the selected dressing product should be evaluated after one week unless there is an adverse reaction to the dressing product.
- Any suspected adverse reaction to the wound dressing product should be reported in the Shift notes and contacted by the client's Care Manager.
Chronic wounds
- A chronic wound fails to follow the normal model of acute wound healing, resulting in delayed or halted closure. Chronic wounds require:
- managing or treating the underlying causes
- assessing and addressing local barriers to wound healing using TIME
- assessing and addressing wider factors delaying healing.
- Examples of chronic wounds include:
- leg ulcers
- pressure ulcers (also called pressure sores, bedsores or decubitus ulcers)
- diabetic foot ulcers.
- Chronic wounds can sometimes require hospitalisation (especially diabetic foot ulcers).
Exudate control
- Controlling exudate is important for comfort, odour, and the prevention of maceration and excoriation of the surrounding skin. Controlling exudate may include:
- a stoma pouch (subject to advice by a specialist health professional)
- suitable absorbent dressings
- skin barrier films or creams to protect the surrounding skin.
- When changing dressings, assess the dressings' exudate-handling capabilities and discuss with the person whether the dressing or frequency of dressings needs to be reviewed.
Odour control
- Odour is often related to the presence of sloughy or necrotic tissue, which leads to an increased bacterial burden and further contributes to problems with odour.
- The most effective way to resolve odour is to treat the cause with debridement and/or reduction of bacterial burden.
- However, this may not be possible or appropriate for every person. Autolytic debridement by maintaining a moist environment is likely the most appropriate method.
- Reducing bacteria levels may involve:
- systemic antibiotics
- topical antibacterial
- antiseptic dressings (may increase pain).
- Charcoal dressings, regular dressing changes, well-sealed/contained dressings, and the use of deodorisers or essential oils applied to the top layer of dressings may also mask the odour.
Bleeding
- Preventing bleeding is a key goal when supporting a person with complex wounds. This is generally achieved by:
- careful dressing application and removal
- maintaining a warm, moist wound bed
- gentle cleansing techniques.
Psychosocial issues
- A person with complex wounds has to deal with not only the pain and discomfort of the wound but also altered body image, reduced mobility and likely deteriorating health.
- It’s important to involve the person’s family and friends according to their wishes.
Pain management
- Severe pain can contribute to poor wound healing, so pain management is essential. Assessing a person’s pain requires considering:
- the wound site
- the frequency of occurrence
- the type of pain
- the severity of the pain
- any relieving or exacerbating factors
- any present analgesia and frequency of administration.
- Knowing this helps identify the likely cause of the pain and how to manage it best. Depending on the situation, pain management may be pharmacological and/or non-pharmacological.
- Carers should seek advice from a health professional regarding pain relief for a person with complex wounds.
- Comprehensive pain management is outside the scope of this policy.
Applies
- when clients are supported with complex wounds
- to all workers, supervisors and key managers supporting clients with complex wounds
Related Items
- Complex Wound Management Prima - Accessible
Policy
Holistic wound assessment
- Holistic wound assessment should be:
- person-centred
- accurate and precise
- able to detect the presence of complications
- able to detect other factors that may delay healing e.g. nutritional status, diabetes, chronic infection and concomitant medication e.g. steroids
- able to provide a framework to monitor the stages of wound healing
- evaluate the effectiveness of any treatment.
- Local wound assessment should be carried out at least monthly and take into account:
- type of wound
- location of wound
- stage of healing—using a recognised scale e.g. pressure ulcer category 1–4, ungraded
- wound dimensions—length, width, depth, position/extent of sinuses, undermining of surrounding skin.
- The client's nutritional requirements should also be assessed to ensure appropriate nutritional needs.
- Consultation with a dietitian may be necessary if the client is at risk of malnutrition.
Inflammation and infection control
- For controlling inflammation and infection:
- follow standard clinical infection control procedures
- maintain good hand hygiene practices
- follow Waste management policy
- systemic antibiotic use should only be decided by a medical practitioner
General care of clients with complex wounds
- As a guide:
- surgical debridement should only be conducted by a qualified and competent health professional
- always choose appropriate and comfortable wound dressings that are trauma-free on removal and take into account odour and the person’s culture and beliefs
- always follow the manufacturer’s instructions when using wound dressings
- combine primary and secondary dressings from the same manufacturer where possible to avoid possible biochemical reactions of combining interactive dressings
- general use of antiseptics/disinfectants is not recommended as these are shown to kill fibroblasts and thus hamper healing
- if a wound fails to respond to treatment, seek advice from a medical practitioner.
Key manager responsibilities when supporting clients with complex wounds
- The responsibilities of key management personnel are to:
- ensure carers have current knowledge and a training plan to teach the standards of care for clients with complex wounds
- provide carer education to provide excellent, confident care
- ensure carers follow the Manage complex wound process
- ensure carers comply with the Medication Policy.
Carer responsibilities when supporting clients with complex wounds
- The responsibilities of carers are to:
- work within their scope of practice and qualifications
- adhere to hand hygiene and infection control policies
- recognise the distinction in a wound between contamination, colonisation and infection
- recognise when a normal inflammatory process, when it becomes abnormal and when it is due to infection
- able to confidently assess, cleanse and dress complex wounds as appropriate
- report incidents via the incident reporting system. refer Incident Management Policy