Guidelines for monitoring falls or incidents to maintain safe and quality services for the client.
What constitutes a fall incident?
A widely accepted definition is “an unplanned descent to the floor with or without injury to the client”. The nursing diagnosis for risk of falls is “increased susceptibility to falling that may cause physical harm".
Some falls are recorded as 'events' as the client was not injured. Perhaps they had poor balance on standing or stumbled on the carpet when mobilising. Other falls are recorded as an 'incident' because they caused minor or major injuries. The increase in stumbling, poor balance, or falls must be recorded in the shift notes, and you may be required to complete a hazard or incident report. Whether the client experiences a fall event or an incident, their mobility confidence is eroded.
When a client experiences a falls incident, HWH will recommend that a physiotherapist or occupational therapist perform a falls risk assessment. The assessment includes a report that contains recommendations to prevent falls. Falls prevention is a difficult outcome to achieve for clients of any care service organisation.
This point of view leads HWH to accept that we can never truly prevent falls, however we can identify and influence risk factors that contribute to client falls. The recommendations that result from the falls risk assessment are used to create a unique Falls Risk Plan for a client to eliminate or reduce the incidence of falls, see our Falls Risk Plan template.
The risk factors that correlate with falls-risk clients are:
balance problems
dizziness or vertigo
medical conditions, e.g., dehydration, diabetes, hypotension, MND, MS, cerebral palsy
medication and drug reactions
falls history
fractures
walking or mobility problems
improper footwear
vision impairment
uneven surfaces
obstacles in walk areas in the home
pets in the home
Older people who fall suffer moderate to severe injuries such as bruises, hip and arm fractures, or head trauma. Severe fractures have been related to an increased risk of death. Falls of older people account for 25% of deaths one year after a severe fall, see references.
What does a HIGH falls risk mean? It means that on every occasion the client rises to stand, they will be at risk of falling due to poor balance, dizziness, hypotension (low blood pressure), medication effects, and/or dehydration. They will require physical assistance to transfer between equipment safely or when using mobility aids, such as a 4WW (4-wheel walker). They are not to mobilise or transfer between equipment alone.
What does a fall risk assessment include?
Older people who present for medical attention because of a fall, report recurrent falls in the past year, or demonstrate abnormalities of gait and/or balance should be offered a multifactorial fall-risk assessment. A physiotherapist or occupational therapist is qualified to assess a person's risk of falling. Consideration of the key risk factors that are common to referral for a fall-risk assessment is below. A fall risk assessment determines if a client has a low, moderate, or high risk of falling. The CCM will arrange a fall-risk assessment if the client presents with the majority of these factors:
A History of falls: all clients with a recent history of falls, such as a fall in the past 3 months, should be considered at higher risk for future falls.
Mobility problems and use of assistive devices: clients who have problems with their gait or require an assistive device (such as a cane or a walker) for mobility are more likely to fall.
Medications: clients on many prescription medications, or patients taking medicines that could cause sedation, confusion, impaired balance, or orthostatic blood pressure changes are at higher risk for falls.
Mental status: clients with delirium, dementia, or psychosis may be agitated and confused, putting them at risk for falls.
Continence: clients with urinary frequency or frequent toileting needs are at higher risk of falls.
Vision impairment could cause a client not to see an environmental hazard, and
Orthostatic hypotension, which could cause the client to become lightheaded or pass out when standing.
Pets in the home
Other client risks include being tethered to equipment, such as an IV pole, that could cause a client to trip while in a hospital or at home.
A fall-risk assessment determines if a client has a low, moderate, or high risk of falling. During an assessment, the following fall assessment tools will be used:
Strength test tool - a handgrip dynamometer is an assessment tool specifically designed to accurately and quantitively measure a person's ability to use his or her forearm and finger flexor muscles to apply a gripping force.
Timed Up-and-Go (Tug). The test starts in a chair, and the client will be asked to stand up, walk for about 10 feet at a regular pace, walk around another chair and then return to sit on the first chair.
30-Second Chair Stand Test. This test checks the strength and balance of a person over a 30-second period; the client stands and sits in a chair with no armrests continuously for 30 seconds.
4-Stage Balance Test. This test checks how well the client can keep their balance.
Falls Risk Assessment Tool (FRAT) - a formal written assessment
Falls Risk Assessment Tool (FRATCOM) - Community - a formal written assessment
Berg Balance Test - standing on one leg and then the other with eyes closed and arms outstretched to the sides, tests if the client is sure-footed with each step, and identifies if the client favours one side of their body when mobilising.
Following the assessments, the physiotherapist or occupational therapist completes a report with recommendations for a Fall Prevention Program for the client, which is stored in the client's Basecamp project>assessments. From this information, HWH develops a Falls Risk Plan, which is stored in the client's Basecamp project>documents and forms part of the client's care instructions.
What is a Fall Prevention?
The most important application of the assessment tools is to identify fall risk factors for which a Falls Risk Plan can be developed. The fall risk assessment scores influence the Falls Risk Plan, which aims to reduce the incidence and severity of falls among older people and/or those with disabilities. It is designed to reduce the social, psychological and economic impact of falls on individuals, families and the community; at HWH we outline fall prevention strategies in the client's Falls Risk Plan.
Each client has a unique risk profile that needs to be integrated into the care instructions that ensure the continuity of care by all staff members.
Fall prevention strategies from a physiotherapist or occupational therapist must be outlined in the mobility and exercises section of the client's care instructions.
The client's care instructions are an active document and are updated regularly. A review of a Fall Risk Plan is completed after a client falls or experiences a significant change in their health or medical condition. Furthermore, the client's care instructions indicate specific actions that should or should not, be performed. All care planning needs to be individualized to fit the client's needs. Each risk factor should have a corresponding plan of care; see our Managing Client's Falls processes.
Falls Risk Plans are stored in the client's basecamp project>documents folder.
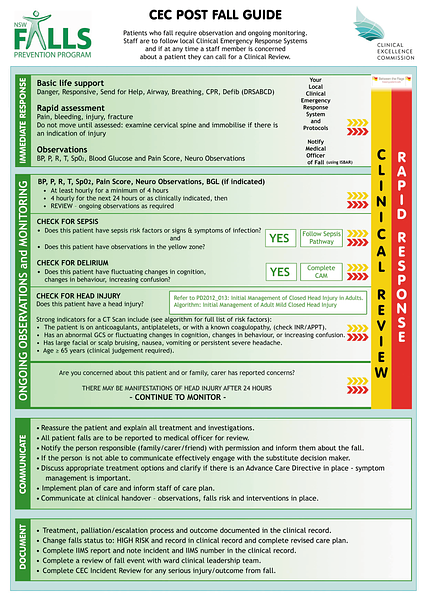
The Clinical Excellence Commission, NSW Government provides the Post Fall Guide as a resource to support clinicians.