Initiating and maintaining both invasive and non-invasive mechanical ventilation is complex.
Workers who have completed training specific to each client's ventilation needs should only use this process and possess the necessary high-intensity support skills required for ventilator management and managing a ventilator-related incident.
Workers supporting clients that require ventilation must:
Become familiar with the ventilator equipment
Know how to use monitoring equipment
know what to do when a ventilator alarm is activated
know what to do in the event of ventilator failure.
Workers must always work within their scope of training and practice. If ever in doubt, seek assistance from your HWH Clinical Care manager or other senior and qualified health practitioner.
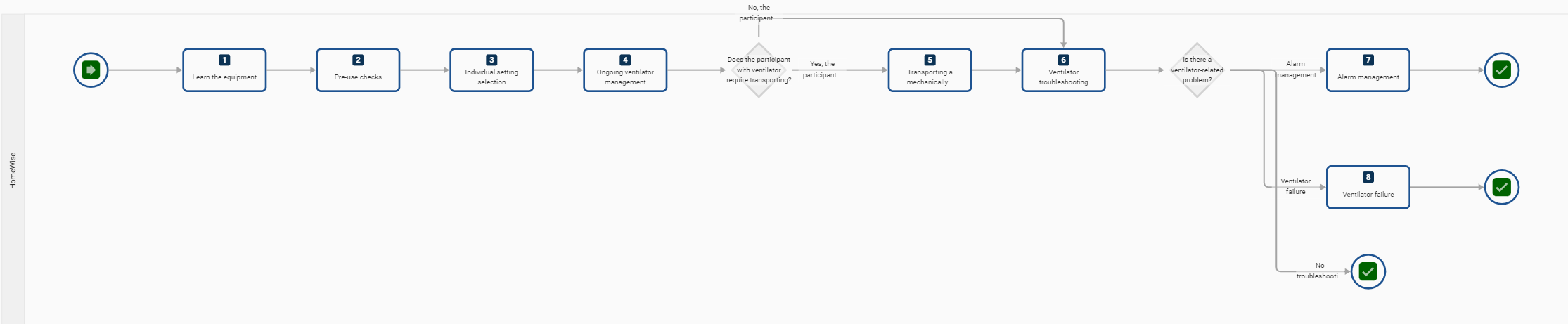
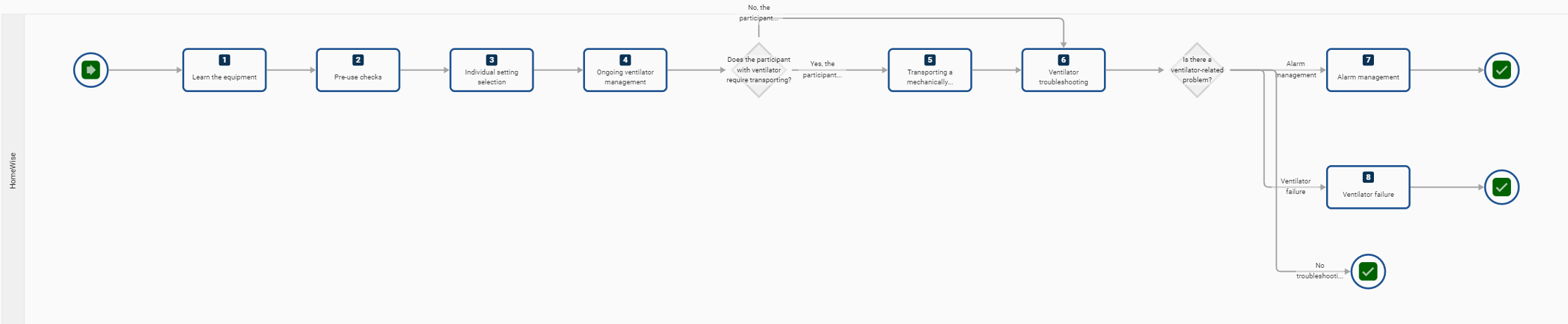
Step 1 - Learn the equipment
It is essential that, before taking responsibility for managing a client who is dependent on a ventilator, you familiarise yourself with that particular equipment:
Ventilatory modes – familiarise yourself with the modes, for example, for switching between IMV, SIMV, PEEP and CPAP
Pressure and volume settings – check that you understand how settings are managed and monitored for inspiratory and expiratory pressure and for tidal volume on this particular machine.
Alarm settings – check that you understand how to set and adjust the alarm settings.
Also, familiarise yourself with the monitoring equipment in use, which may include:
Pulse oximetry – SaO2 is routinely carried out for patients on ventilators via digital pulse oximeters, and you need to be familiar with the machine being used for this patient
Capnography – End-tidal CO2 may be monitored via a capnograph—be familiar with this device.
Step 2 - Execute Pre-Use Checks
Pre-use checks are to:
Conduct a full ventilator pre-use check before deploying the machine for use with a client
While modern ventilators have a self-test at power-up, additional pre-testing is necessary to ensure safe ventilator operation before placing on a client
The pre-use check confirms the function and integrity of the ventilator circuit, including the internal ventilator components, tubing and the humidifier system
The pre-use check should be performed during the circuit or humidifier setup.
NOTE: Complete this test anytime the ventilator circuit is changed or modified.
Step 3 - Individual Setting Selection
When powered up, some ventilators default to generic, predetermined settings, while others default to the last operational settings. Depending on their needs, the default settings may present a hazard to the client.
The prescribed patient-specific ventilator settings must be recorded accurately, comprehensively and legibly in the participant’s ventilator management plan.
Before being deployed, the ventilator must be adjusted to the client’s specific, prescribed settings for:
pressures
volume
FiO2
rate.
If there are any concerns about the functioning of the ventilator, do not proceed to deployment. Instead, arrange alternate measures and report the fault to the Clinical Care Manager or the ventilator maintenance professionals.
Step 4 - Ongoing Ventilator Management
Ventilator settings:
Must not be changed unless authorised by the responsible clinician and accompanied by a written prescription
maintain effective communication between all support workers and responsible health professionals to ensure settings are correct, clear and understood by all parties
appropriate assessments of SaO2 and CO2 should be maintained and recorded in writing at regular intervals
workers must remain vigilant to any changes in the client's condition, such as:
hypoxia
hypercapnia
respiratory effort
respiratory resistance
reduced cardiac output
patient distress
Any change made to the client’s ventilator settings must be accompanied by a full assessment of the person’s condition to determine the effect of the change
where invasive ventilation is in use, after the person is moved for any reason, bi-lateral auscultation of breath sounds should be carried out by a health professional to establish if there has been no movement of the ET tube
If the client has a tracheostomy tube in place, you may also refer to the Managing a Tracheostomy process to support this person.
Decision A: - Does the client require transporting
Yes - Step 5 - Transporting the mechanically ventilated
No - Step 6 - Ventilator Troubleshooting
Step 5 - Transporting the mechanically ventilated
When transporting a mechanically ventilated client:
Clients who are chronically ventilated may be transported with one qualified worker with a second worker supporting if the circumstances require it
Clients must be transported with a transport ventilator or manually ventilated with a manual ventilation device (MVD)
If using a transport ventilator, ensure additional batteries are available and that it is plugged into the power when available
Clients with an endotracheal tube or tracheostomy should have all supplies that would be required for re-intubation - this includes an intubation kit and bag-valve-mask with PEEP valve
an oxygen source with a reserve of 30 minutes longer than is required—it’s preferable to conserve transport oxygen and use an alternate oxygen source if one can be obtained from a non-transport source if the client is having tests or a medical procedure
All mechanically ventilated clients require SaO2 and ETCO2 monitoring during transport.
Step 6 - Ventilator Troubleshooting Decision B: Is there a ventilator-related problem?
Alarm Management - Step 7
Ventilator Failure - Step 8
No troubleshooting is required at present - End
Step 7 - Alarm Management
If a ventilator alarm has been activated, promptly attend to the alarm and determine the core reason for the activation.
Correct monitoring and setting of the ventilator alarms can save lives!
Establishing appropriate and safe strategies for ventilator alarm management is critical to caring for clients with mechanical ventilation.
Good alarm management practices include:
comprehensively and legibly documenting alarm settings in the client's ventilator management plan
maintaining alarm settings on ventilatory settings as well as volume, pressure and rate, SaO2 and CO2
set alarms to a specific percentage of the ventilator settings—if the client’s ventilator management plan does not have these settings, clarify what alarm settings are best with the responsible health professional
Check the alarm settings:
at ventilator setup and deployment
at the start of each shift
at regular intervals during each shift
Make every effort to establish good routines to mitigate nuisance alarms and alarm fatigue.
Go to End Step 8 - Ventilator Failure
A backup ventilation plan is essential in the event of ventilator failure.
A backup ventilator is required, and equipment is to ‘handbag’ the client until alternate equipment is installed.
In the event of ventilator failure:
ensure the patient maintains adequate respiratory effort until the backup plan is implemented, e.g. backup ventilator
In the invasive ventilation of an unconscious client, this may require hand-bagging with an Ambu bag (manual resuscitator) and oxygen supply
monitor the client's condition closely and record their clinical parameters
Report immediately to the responsible health professional or call an ambulance

{kind=link}