This policy aims to assist HWH, clients, and other stakeholders in managing mealtimes effectively and safely, using best practices to minimise the risk for persons with nutritional issues or swallowing difficulties (Dysphagia) in the community setting. HWH follows the International Dysphagia Diet Standardisation Initiative Framework (IDDSI Framework).
Support workers may work with people who require mealtime assistance and follow written meal preparation and delivery instructions.
They require relevant training, although this work typically requires something other than specialist skills.
Providers will support their workers and others involved in providing support to
Read, interpret and implement mealtime management plans;
Follow food preparation procedures;
Deliver food and monitor eating to identify and respond to risks;
Arranging/supporting postural requirements.
Providers will deploy staff with knowledge of
signs and symptoms of swallowing and feeding difficulties;
risks associated with eating and swallowing;
risks associated with not following the mealtime plan;
food preparation requirements and methods for common conditions e.g. people with dysphagia;
awareness of procedures and methods for including medication in food where this is required by the plan, including an understanding of crushable/non-crushable medication;
common terminology related to mealtime preparation and modified meals.
Background
In 2019, an Australia-wide research project and scoping review on the prevalence of and factors contributing to the deaths of people with a disability was conducted by the National Disability Insurance Commission.
Respiratory disease was the major underlying cause of death for people with a disability across the reviewed reports.
Aspiration pneumonia was the most common underlying cause of respiratory death, accounting for just under half of all respiratory deaths.
The following factors were reported as contributors to these outcomes:
safe mealtime guidelines were not consistently being adhered to due to
lack of staff knowledge and, or understaffing of dysphagia;
high rates of psychotropic prescriptions and polypharmacy;
increasing risk of impaired swallowing function;
sedation and hypersalivation;
delays in diagnosis and treatment of respiratory-related illness;
lack of timely access to influenza and pneumococcal vaccines, and lack of comprehensive
nutrition and swallowing assessments for at-risk groups.
Across the reports, accidental choking was highlighted as the leading external cause of death for people with disabilities.
People with lifelong health conditions or disabilities have a higher incidence of dysphagia.
The impacts of dysphagia are widely reported and can be serious, long-lasting and substantial (Bryant & Hemsley, 2018).
Dysphagia and mealtime interventions can impact a person’s quality of life, well-being, and participation across the lifespan.
Scope
This policy applies to the management of dysphagia at mealtimes of all HWH clients, including the administration of oral medication.
Desired Outcome
To maintain a quality and safe standard of service delivery support
To proactively reduce the number of deaths attributed to choking and respiratory infections in persons with a disability, due to the lack of understanding in the identification and prevention of such incidents, by early identification of a person at risk and implementing strategies to prevent their harm.
Definitions and Supporting Information
Speech Pathologist/ Speech Therapist/Speech Language Therapist is a health professional trained to assess, diagnose, and treat communication, swallowing, speech, language or voice disorders.
A (Home) Support Worker is an individual who assists or supervises a client in performing tasks of daily living to support and maintain general well-being and enable meaningful involvement in social, family, and community activities in the person’s home and community. The Support Worker is a paid person with access to education, support and advice from the Service Provider line manager or team leader.
A Support Worker is also commonly known as an attendant care worker, disability worker, aged care worker, community worker, home care worker, care worker or paid carer.
A Support Worker with Mealtime Management Competency is a support worker trained and assessed as competent by a skilled registered nurse, allied health professional or a person deemed competent by HWH to safely and appropriately perform a specified task as a support worker.
Aspiration is when food, fluid or saliva enters the airway and, or lungs before, during or after swallowing. This can occur with obvious signs and symptoms or silently.
A carer is a person who provides care to the client at no cost (generally family or friends).
Community Support and, or Services are defined as the provision of paid support and services in a client's home or community.
Dysphagia is a medical term for any difficulty in the swallowing process of food or fluids. It may include:
weakened muscles or lack of muscle coordination, which makes managing food or fluid in the mouth difficult;
poor initiation of the swallow;
slowed or absent reflexes such as cough;
reduced or no sensation in the airway;
incoordination of the swallow
structures in the pharynx or larynx.
A person may have dysphagia due to poor posture, varied levels of alertness, cognitive impairment, or aging.
Dysphagia can be caused by neurological conditions such as Stroke, Traumatic Brain Injury, Cerebral Palsy, Parkinson’s Disease, Motor Neurone Disease and other degenerative diseases. People with intellectual disabilities can also have dysphagia.
Early signs of dysphagia may be coughing, throat clearing, gagging, or choking while eating and drinking. This could mean the person is aspirating (see definition), which can cause pneumonia.
Other signs of dysphagia are repeated or unexplained chest infections and, or raised temperature, unexplained weight loss, dehydration, weak or absent cough or swallowing, or drooling.
Further signs and symptoms of potential dysphagia are:
eating takes longer than normal;
the need to cough or clear the throat during or after eating and drinking;
frequent complaints of heartburn;
shortness of breath when eating and drinking;
avoidance of some foods because they are hard to swallow.
Babies that have difficulty sucking during breast or bottle feeding could have dysphagia.
Instrumental swallowing assessment: While the above signs and symptoms of dysphagia are important and should be reported immediately, they are not always reliable indicators of aspiration.
The gold standard for aspiration detection is instrumental swallowing assessment, such as a videofluoroscopic swallow study (a moving x-ray of swallow function).
Persons with a disability should be referred for instrumental swallowing assessment by a treating medical practitioner where appropriate.
A speech pathologist and radiologist should conduct the instrumental swallowing assessment.
Dysphagia Treatment
The most appropriate treatment for dysphagia will depend on its cause and presentation. Treatment and management plans should be tailored to individual service users by a specialist in dysphagia management who can assist with:
modifying textures of foods or drinks
swallowing techniques or strategies focusing on positioning or placement of food
exercises or stimulation
medication to reduce stomach acid reflux or relax the oesophagus
In some cases, enteral feeding may be indicated to augment or replace an oral diet.
CCMs ensure mealtime and medication assistance practices relate to a client's dysphagia management.
Food and fluid may be modified at the instruction of a speech pathologist based on swallow assessment results. Changing the texture of food and the thickness of fluids can assist the person in swallowing safely and minimise the risk of aspiration. However, textured diets and thickened fluids are prescribed by a speech pathologist, not a nurse or support worker. Ensure you notice any changes in the client's swallowing skills immediately for a review of the MMP by a speech pathologist.
“Since May 1, 2019, Australia has followed the International Dysphagia Diet Standardisation (IDDSI) Framework. This is a change from the Australian Food Texture Scale previously utilised.”
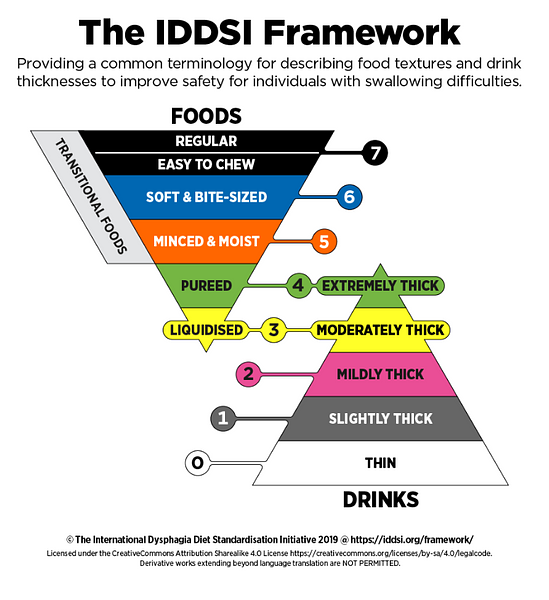
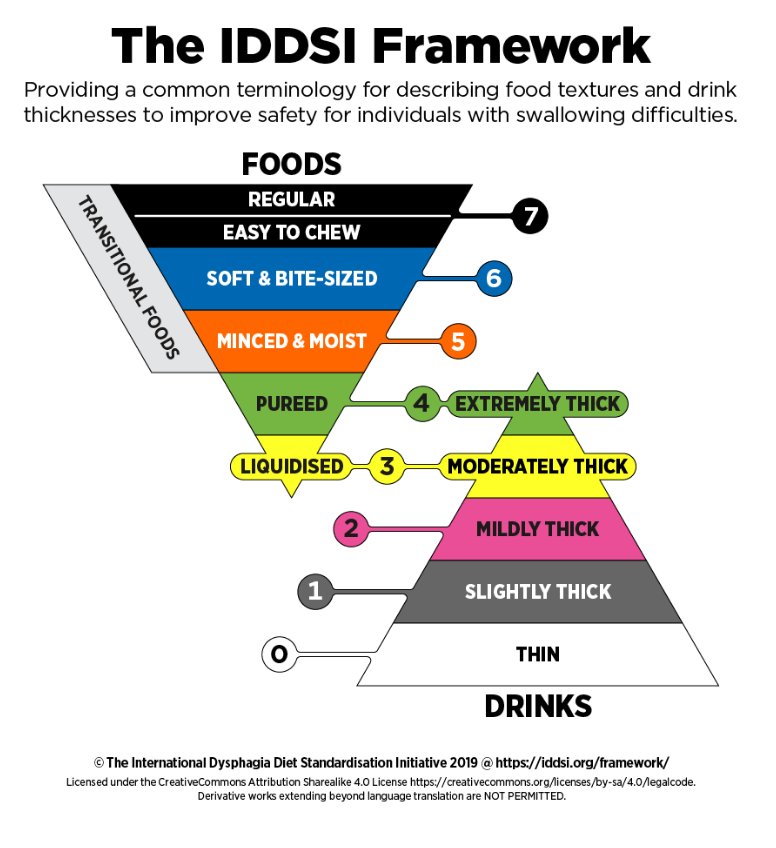
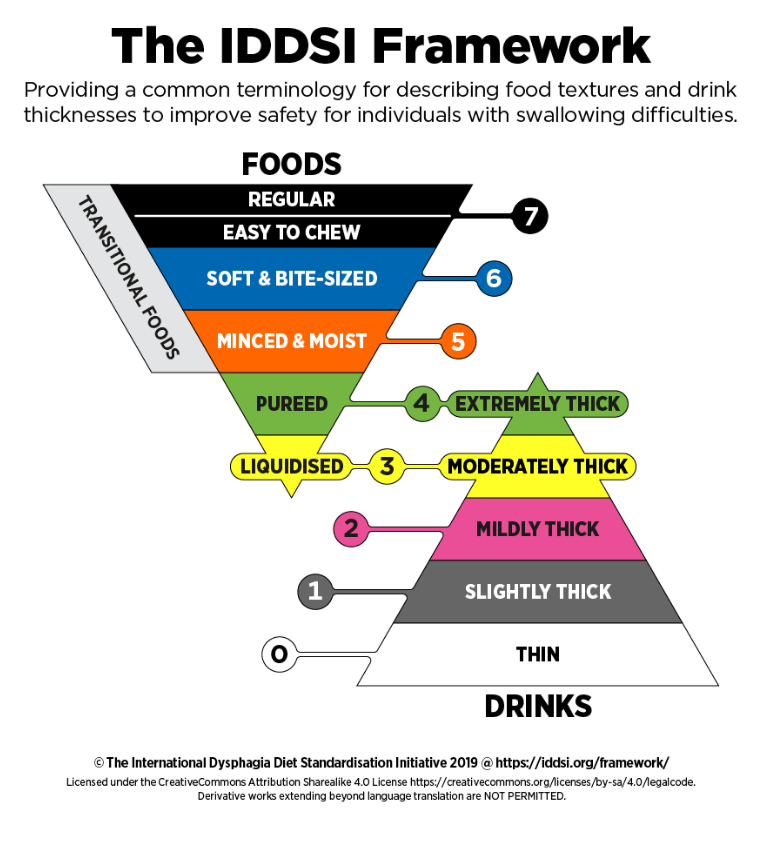{kind=link}